Predictors of development of chemical pneumonitis among children admitted in pediatric emergency ward of Burdwan medical College with ingestion of liquid hydrocarbon
Original Article
Original Article
![]()
Abstract:
Background & Objectives: Informations regarding predictors for development of chemical pneumonitis among children who ingested hydrocarbon are scarce in Indian context. Hence this study was undertaken to find out the factors responsible for development of chemical pneumonitis among children admitted with ingestion of liquid hydrocarbon in pediatric emergency ward of Burdwan Medical College, Bengal.
Mehodology: A hospital-based study was conducted among 173 children selected by complete enumeration method with a mean age of 4.81±2.48 years. Chi-square test and binary logistic regression method was used to find significance of association between different variables and chemical pneumonitis.
Result: 38.15 of the study population developed chemical pneumonitis. Majority of them were from to rural area (68.2%),ingested more than 30 ml of hydrocarbon (80.3%), hospitalized more than 2 hours after ingestion (69.7%), not treated with hydrocortisone (75.8% & 71.2%, respectively) and developed fever within 1st 2days after ingestion(84.8%).Our model predicted 96% of dependent variable correctly.
Conclusion: Proper treatment protocol should be developed for treatment of hydrocarbon ingestion. Appropriate preventive measures should be taken to prevent ingestion of hydrocarbon.
Keywords:Kerosine poisoning, chemical pneumonitis
Introduction:
Liquid Hydrocarbon ingestion is the most common mode of poisoning in children of low & middle-income countries like India.1 One study in Africa estimated that cost of hospitalization due to ingestion of hydrocarbon is approximately 1.4 million US $ per year.2 Ingestion of liquid hydrocarbon may lead to development of a distinct type of chemical pneumonitis, also known as Fireeater’s pneumonia.3,4 Almost half of the children may develop this complication following ingestion of hydrocarbon.5 Different studies had identified use of corticosteroid(either intravenous or inhalational or both) & nebulisation with salbutamol/ levosalbutamol as important treatment which protect from development of chemical pneumonitis following ingestion of hydrocarbon.6 But these type of studies are scarce in Indian scenario. Hence this study was undertaken to find out the efficacy of different modes of treatment in preventing development of chemical pneumonitis in patients who ingested liquid hydrocarbon.
Methodology: This hospital-based study was conducted in the pediatric emergency ward of Burdwan Medical College, Burdwan from May 2016 to October 2016. All children who were admitted for liquid hydrocarbon ingestion were included, following complete enumeration method. Total 179 children were admitted for hydrocarbon ingestion, but six were excluded from the study (3 for not giving consent, 2 were discharged on risk bond and 1 patient had congenital heart disease from which he died). Hence, a total of 173 children were studied. Data were collected by reviewing hospital record as well as clinical examination of admitted patients. Single stethoscope is used throughout the study for quality control. X-ray plates of each patient who developed chemical pneumonitis was reviewed twice by two different radiologists.
Operational Definition: Chemical pneumonitis cases were defined as who developed tachypnea, fever or have distinct radiological abnormality in form of unilateral or bilateral consolidation and/or pneumatocele formation.7
Statistical Analysis: Collected data were put in Microsoft excel worksheet. Mean values are used for continuous data, whereas categorical data are expressed in proportion. Chi-square (χ2) test was used to assess significance of association between two attributes in contingency tables. Degree and direction of relationship between two variables was computed by Pearson’s product moment correlation co-efficient (r). Scores were assigned for categorical variables (Rural-0, urban- 1; hydrocortisone not used-0, used-1; Nebulisation not used-0, used-1; amount of ingestion: <10ml-1, 10ml-30 ml-2,>30ml-3; time between ingestion & hospitalization: <1 hour-1, 1-2 hour-2, >2 hour-3; presence of fever in 1st 2days: absent-0, present-1)) A logistic regression model (forward conditional method) was also generated using development of chemical pneumonitis [not developed (0) / developed (1)], as the outcome / dependent variable. Amount of ingestion, time between ingestion & hospitalisation, presence of fever in 1st 2 days after ingestion & use of nebulisation were entered in step 1, 2, 3 & 4, respectively. P< 0.05 was considered statistically significant. All the statistical analysis was done in SPSS software, version 19.0 (Statistical Package for the Social Sciences Inc, Chicago, IL, USA).
Result: Mean age of the study population (n=173) was 4.81±2.48 yrs. Females are 52.6%, rest are male (43.4%). 58.9% of them are from rural population & maximum (54.9%) of them belong to middle class according to modified BG Prasad Scale8.Kerosene was the most frequently (89.0%) ingested substance, followed by terpene and others(diesel, petrol, glycerol etc).38.1% of study population developed chemical pneumonitis subsequently. Most commonly affected lobes are both lower lobes (38.1%), followed by left upper lobe (22.6%).
Chemical pneumonitis more commonly develops among rural patients (68.2%), who ingested more than 30 ml of hydrocarbon (80.3%), who are hospitalized more than 2 hours after ingestion (69.7%), in whom hydrocortisone & nebulisation were not used (75.8% & 71.2%, respectively) and who developed fever within 1st 2days after ingestion(84.8%).On the other hand it is less commonly developed among urban patients(53.7%), who ingested less than 10 ml of hydrocarbon(81.3%), who are hospitalized within 1 hour after ingestion(79.4%), in whom hydrocortisone & nebulisation were used (88.8% & 84.1%, respectively) and who did not develop fever within 1st 2days after ingestion (81.3%). All these associations are found to be statistically significant. (Table 1) On the other hand, there is no statistically significant association between development of chemical pneumonitis with age, sex, socioeconomic status, type of ingested hydrocarbon & use of antibiotic.
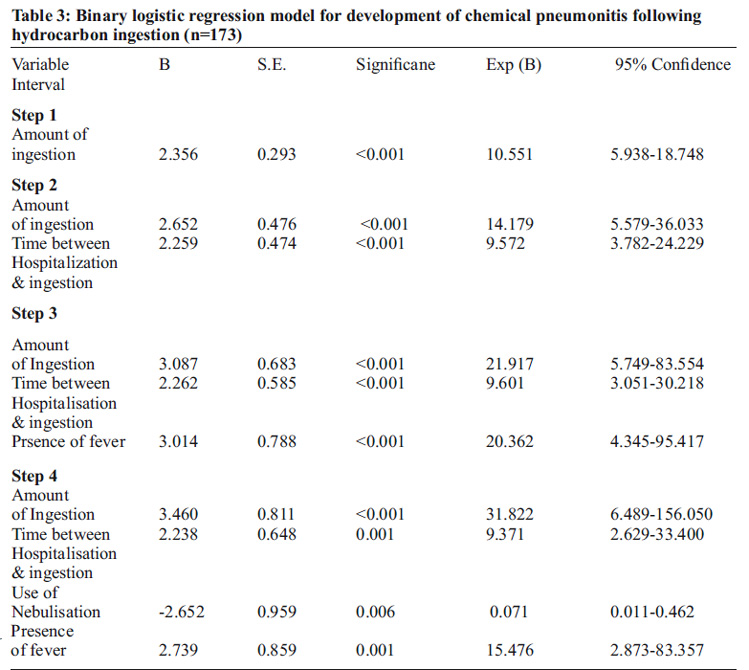
There is statistically significant positive correlation of chemical pneumonitis with amount of hydrocarbon ingestion (0.780), time between ingestion and hospitalization (0.686) and presence of fever (0.646). Whereas, correlation of chemical pneumonitis with use of nebulization and hydrocortisone (-0.557 & -0.654) respectively is statistically significant but negative, i.e. they are protective. Though urban residence seems to be p r o tectiv e in d ev elo p men t o f ch emical pneumonitis, correlation is insignificant statistically (Table 2). Chemical pneumonitis is 31.8 times more likely to develop in children who ingested higher amount of hydrocarbon. It also more likely develops among children who were hospitalized in late (Adjusted odds ratio: 9.4) & who developed fever in 1st two days after ingestion (Adjusted odds ratio: 15.5). On the other hand, nebulisation with salbutamol/levosalbutamol found to be protective , having an adjusted odds ratio of 0.07. Use of hydrocortisone, though significantly correlated with development of chemical pneumonitis among the patients, become insignifacnt in the binary logistic regression model. (Table 3) Amount of ingestion, time between ingestion & hospitalization, use of nebulisation & presence of fever in 1st 2days- these four variable can explain 66.7% to 90.7% variance of development of chemical pneumonitis among the study subjects. Overall, our model can correctly predict 96% of the outcome variable.
Discussion:
Lifshitz M5et al found that 43% of children who ingested kerosesne developed chemical pneumonitis, which is slightly larger than our finding (38.1%). Karim RM9et al found that 52% victims of accidental ingestion of kerosene develops chemical pneumonitis later on. Similar to the finding of Basu M10et al, we also found that kerosene is the most common culprit (in 89% cases). Konca C11et al found inhalational or intravenous hydrocortisone is protective and prevents chemical pneumonitis. Similarly we also found that used of hydrocortisone protects the patients from development of chemical pneumonitis. Balme KH12et al in a randomized control trial showed that antibiotic has no role in treatment of chemical pneumonitis. We also noted similar finding. But use of antibiotic may be justified, because chemical pneumonitis also has similar signs and symptoms of bacterial pneumonia, and in the early days they are very difficult to differentiate. Moreover, Singh H13et al also found that antibiotic like Carbencillin may decrease morbidity. Ahmed B14et al found that lower socio economic status as a risk factor, but we do not find any significant relationship with it.
Conclusion:
The main limitation of this study is small sample size. But it may help to develop appropriate treatment protocol for liquid hydrocarbon ingestion.
Preventive measures should be taken in form of child-resistant packaging15, legal measures16 and proper education17,18 of the parents for prevention of ingestion of liquid hydrocarbon, so that this grave problem is eliminated at the root.
Contribution of Authors:
KI: collection of data, writing manuscript, statistical analysis, AKD: Concept of Study, Revising manuscript, gurrantor, AR: Revising manuscript, RD: Revising manuscript, SS: Collection of data
Conflict of Interest: None
Source of Funding: Self.
References:
1. Dutta AK, Seth A, Goyal PK, Aggarwal V, Mittal SK, Sharma R, Bahl L, Thakur JS, Verma M, Chhatwal J, Chacko B, Saini V, Singhal A, Sharma P, Sharma U,Chaturvedi P, Kumar S, Prajapati NC, Vaidya J, Garg N, Basu SN, Lahiri M, Das CK,Pal DK, Lall SB, et al. Poisoning in children: Indian scenario. Indian J Pediatr.1998 May-Jun;65(3):365-70.
2. Danseco ER, Miller TR, Spicer RS. Incidence and costs of 1987-1994 childhood injuries: demographic breakdowns. Pediatrics. 2000 Feb;105(2):E27
3. Lizarzábal Suárez PC, Núñez Savall E, Carrión Valero F. Lipoid pneumonia due to accidental aspiration of paraffin in a “fire eater”. Arch Bronconeumol. 2015 Oct;51(10):530-1.
4. Franquet T, Gómez-Santos D, Giménez A, Torrubia S, Monill JM. Fire eater’s pneumonia: radiographic and CT findings. J Comput Assist Tomogr. 2000 May-Jun;24(3):448-50
5. Lifshitz M, Sofer S, Gorodischer R. Hydrocarbon poisoning in children: a 5-year retrospective study. Wilderness Environ Med. 2003 Summer;14(2):78-82
6. Raghavendran K, Nemzek J, Napolitano LM, Knight PR. Aspiration-induced lung injury. Crit Care Med. 2011 Apr;39(4):818-26.
7. Bulava A, Kolek V, Lukl J. Fire-eater’s pneumonia–a difficult differential diagnosis. Cas Lek Cesk. 2001 Apr 26;140(8):242-5
8. Mangal A, Kumar V, Panesar S, Talwar R, Raut D, Singh S. Updated BG Prasad socioeconomic classification, 2014: a commentary. Indian J Public Health. 2015 Jan- Mar;59(1):42-4
9. Karim RM, Momin IA, Lalani II, Merchant SS, Sewani AA, Hassan BS, Mahmood N.Aspiration pneumonia in pediatric age group: etiology, predisposing factors and clinical outcome. J Pak Med Assoc. 1999 Apr;49(4):105-8
10. Basu M, Kundu TK, Dasgupta MK, Das DK, Saha I. Poisoning, stings and bites in children- – what is new? An experience from a tertiary care hospital in Kolkata.Indian J Public Health. 2009 Oct-Dec;53(4):229-31
11. Konca C, Tekin M, Turgut M. The Combined Use of Inhaled and IntravenousSteroids for Children With Chemical Pneumonitis After Ingestion of Paint Thinner.Iran Red Crescent Med J. 2016 May 15;18(7):e24300
12. Balme KH, Zar H, Swift DK, Mann MD. The efficacy of prophylactic antibiotics in the management of children with keroseneassociated pneumonitis: a double-blind randomised controlled trial. Clin Toxicol (Phila).2015;53(8):789-96
13. Singh H, Chugh JC, Shembesh AH, Ben-Musa AA, Mehta HC. Management of accidental kerosene ingestion. Ann Trop Paediatr. 1992;12(1):105-9
14. Ahmed B, Fatmi Z, Siddiqui AR, Sheikh AL. Predictors of unintentionalpoisoning among children under 5 years of age in Karachi: a matched case-control study. Inj Prev. 2011 Feb;17(1):27-32.
15. O’Brien C. Pediatric poisoning fatalities from 1972 to 2005. Bethesda, MD: US Consumer Product Safety Commission; 2008. [8 April 2008]
16. SI No. 462/2998 – European Communities (Dangerous substances and preparations) (Marketing and use) Regulations. European Commission; 1998. [6 April 2008]
17. Donald PR, Bezuidenhout CJ, Cameron NA. An educational campaign in the Cape Town area to prevent paraffin poisoning. South African Medical Journal. 1991;79:281–282.
18. Woolf AD, Saperstein A, Forjuoh S. Poisoning prevention knowledge and practices of parents after a childhood poisoning incident. Pediatrics. 1992;90:867–870.


Issue: April-June 2017 [Volume 6.2]