Pediatric Radiology Review
Radiology Review
Radiology Review
![]()
Interpretation of X-Ray Chest :
Interpretation of X-ray Chest is of immense importance in pediatric practice.Although sophisticated gadgets are very much use in our day to day practice yet role of conventional radiographic examination cannot be ignored rather still remains the corner stone of basic investigation. Plain & Fluoroscopy constitute 80-85% of paediatric study.And other investigations like USG(8-12%),CT (3-5%), MRI(2-4%), Nuclear Medicine(2-4%)and Vascular & interventional Procedure (0.5-1%) contribute the rest.Among plain X-rays, Chest X-ray takes its share of 65 to 70%. So one must know how to read Chest x-rays properly and methodically.
Abcs Of Interpretation Chest X-ray
- A—–Abdomen
- B—–Bones
- C—–Chest
- S—–Soft tissues
So everybody must learn a methodical approach so that it becomes routine practice and thus missing findings may be minimised.
Reading CXR’s
- Have a structured method!
- Be consistent with that method
- Please don’t take short cuts
- Look at all your patients xrays yourself
- Practice…Practice… Practice
Chest X-ray
- Views- PA, Lat, AP, lateral decubitus ( oblique view– in cardiac investigation ).
- Steps of interpretation (from outside inward )
- soft tissue shadows
- bones
- domes of diaphragm
- trachea
- cardiac silhouette
- superior mediastinal & hilar shadows
- costophrenic sulci
- lung fields
This approach of reading Chest X-Ray will be very helpful as chance of missing even subtle findings would be narrow.

Adequacy of a skiagram
One should be able to count 10 posterior and 6 anterior ribs in Supine AP view
Three Main Factors Determine the Technical Quality of the Radiograph
- Inspiration
- Penetration
- Rotation
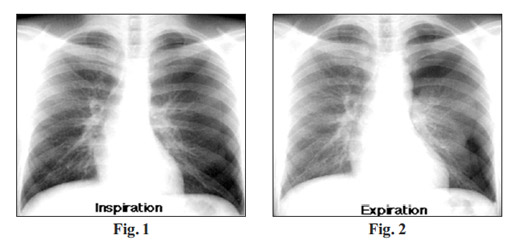
Inspiration
The chest radiograph should be obtained with the patient in full inspiration to help assess intrapulmonary abnormalities.
At full inspiration, the diaphragm should be observed at about the level of the 8th to 10th rib posteriorly, or the 5th to 6th rib anteriorly
Expiratory film is required to diagnose
- Pneumothorax
- Foreign bodies
Expiration reduces lung volume, making a small pneumothorax easier to see.
Penetration
a properly exposed chest radiograph:
- The lower thoracic vertebrae should be visible through the heart
- The bronchovascular structures behind the heart (trachea, aortic arch, pulmonary arteries, etc.) should be seen
Prerequisites For Proper Chest X-ray

Frontal film
Both pedicles of spine and Broncho-vascular markings Should be visible through
Cardiac shadow
- Lateral film :
More caudal thoracic vertebral
Underexposure
In an underexposed chest radiograph, the cardiac shadow is opaque, with little or no visibility of the thoracic vertebrae.
The lungs may appear much denser and whiter, much as they might appear with infiltrates present.
Over exposure :
With greater exposure of the chest radiograph, the heart becomes more radiolucent and the lungs become proportionately darker.In an overexposed chest radiograph, the air-filled lung periphery becomes extremely radiolucent, and often gives the appearance of lacking lung tissue, as would be seen in a condition such as emphysema.

Rotation
Patient rotation can be assessed by observing the clavicular medial heads and determining whether they are equal distance from the spinous processes of the thoracic vertebral bodies.

Now you must learn how to read out a normal Chest X-Ray. It should be methodical and structured.Vig.
X-ray chest PA view shows normal soft tissues, visualized bones and the diaphragm. Trachea is central in position. Cardiac silhouette appears normal. Superior mediastinal and hilar shadows appear normal. Costrophrenic angles are clear.Lung fields are clear. No other significant finding.
Impression: Normal appearance.
Issue: January-March 2018 [Volume 7.1]