Effect of Vitamin D supplementation onAnthropometric measures in exclusively breast fed infants
Original Research
Original Research
![]()
Abstract:
Objective : 1) To study effect of Vitamin D3 supplementation on Anthropometric Measures (Nutrition). 2)To compare above mentioned Parameter in 2 groups namely Vitamin D3 Supplemented Exclusively breastfed infants and Vitamin D3 not supplemented exclusively breast fed infants. Methods: A randomized control study was conducted in 200 new borns, who were exclusively breast fed . New borns were divided into two groups namely Group A- placebo, Group B- vitamin D supplemented i.e. 400 IU daily per orally for 9months . Both the groups were followed at regular intervals 1.5, 2.5, 3.5, 6, 9 months. At each visit anthropometric measurements (weight and length) were recorded. Results: The mean birth weight and length of subjects in Group A and B was comparable (p>0.05). No difference in Anthropometric parameters were noted between two groups at 1.5 month. Significant difference in Anthropometric measures was seen between the above mentioned groups at 2.5 , 3.5, 6 and 9 months (p<0.05). Conclusion: significant improvement in anthropometric parameters from 2. 5 months onwards was seen in Group B subjects , who were supplemented with vitamin D as compared to Group A.
Key words: vitamin D supplementation, anthropometry,exclusively breast feed baby
Introduction: Vitamin D is an essential nutrition component having unique metabolism and physiological effects compared to other vitamins; in fact, it is more suitable to be classified as a hormone1-5. In humans, vitamin D is synthesized in the skin from exposure to sunlight or can be obtained through dietary intake that functions as a steroidal hormone after conversion in the renal tubule to its active form 1-25-hydroxyvitamin D (25(OH)D) by 1-alpha-hydroxylase enzyme. It is a well-known fact that natural sources of vitamin D in foods are not adequate for normal body requirements. Therefore, formation of vitamin D through exposure to sunlight in skin is the major source of vitamin D6,7 . Vitamin D has evolved into a hormone that is active throughout the body not only to regulate calcium and bone metabolism but also to reduce the risk of chronic diseases including auto immune diseases, malignancies, cardiovascular and infectious diseases. Though majority of population in India lives in areas receiving ample sunlight throughout the year, vitamin D deficiency is very common in all the age groups and both the sexes across the country. The immunomodulatory properties of vitamin D may influence susceptibility to infection. Although appropriate levels for immunologic function have yet to be identified, vitamin D deficiency in relation to skeletal metabolism for children is defined as a serum 25(OH)D level <50 nmol/L . Vitamin D is a fat-soluble vitamin that is converted to a hormone within the body. Hormones are considered to be the chemical messengers that relay messages to cells by expressing specific sequences of deoxyribonucleic acid (DNA), which is contained within the cell nucleus. The cell then responds through the process of transcription and translation and produces specific proteins, which then perform direct functions in the Body.8 The active form of vitamin D, calcitriol, acts as a hormone by binding to vitamin D receptors (VDRs) both on the cell membrane as well as in the nucleus. This binding then leads to specific gene expression 9. The skin synthesizes a steroid, 7-dehydrocholesterol, which is isomerized to vitamin D3 , cholecalciferol. Vitamin D3 diffuses into the blood stream reaches the liver,and gets hydroxylated, becomes 25 hydroxy vitamin D. It is then transported to the kidney and converted to 1,25 hydroxyvitaminD3 which is the active form of vitamin D.
Methods:
A randomized control study was conducted at Department of Pediatrics, MGM hospital, Kalambolli, during period of 6 months from 1st march 2014 to 30 September 2014 and followed up till 30 june 2015. All full term newborns delivered in hospital during study period and fulfilling eligibility criteria were included in study after taking informed consent from parents. A final sample of 200 newborns, were then randomized into two groups: Group A: Placebo group and; Group B: Vitamin D3 supplementation group (400IUOD). Both the groups were followed up at regular intervals (1.5, 2.5, 3.5, 6 and 9 months) during which anthropometric measurements (weight and height) were monitored.
Results:
1. The mean birth weight and height of subjects in Vitamin D (Group B) and Placebo group (Group A) was comparable (p> 0.05). Table1
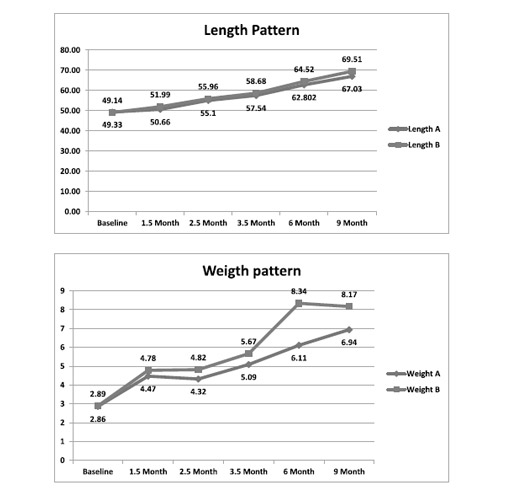
2. No difference in anthropometry parameters was noted between 2 groups at 1.5 months. Table2
3. Significantly better anthropometry parameters were noted in vitamin D group of babies as compared to placebo group (i.e. more weight gain and increased height) from 2.5 months of age (p<0.05). Table 3
Difference in anthropometric parameters was noted between two groups at 3.5 months, 6 months and 9 month .(p<0.05) Table 4,5,6.

The mean birth weight and height of subjects in Vitamin D (Group B) and Placebo group (Group A) was comparable (p> 0.05). This ensured that any difference (if noted) in anthropometry parameters during subsequent visit could not be attributed to differences in baseline parameters.


Significantly better anthropometry parameters were noted in vitamin D group of babies as compared to placebo group (i.e. more weight gain and increased height) from 2.5 months of age
Discussion :
We observed significantly better growth in vitamin D group of babies as compared to placebo group (i.e. more weight gain and increased height) from 2.5 months of age. The significant benefit of vitamin D supplements for these infants on length and weight is an important finding. Stunting is common in many low income populations, starts early in life, and is largely irreversible.10 Stunting has also proved difficult to prevent, possibly because of the large number of related nutritional, infectious, social, and environmental factors.
In a study by Kumar et al. effect of vitamin D3 supplementation on mortality and morbidity of low birth weight infants was observed. They observed that vitamin D treatment significantly increased standard deviation (z) scores at six months for weight, length, and arm circumference and decreased the proportion of children with stunted growth (length for age z score ?2) or with arm circumference z scores of 2 or less 11.
Mazary et al. also observed a positive corelation between Vit. D3 supplementation and anthropometric measurements in full term infants12.
In a similar study by Brook et al. weight of the new borns remained approximately equal between the groups at 3 month and began to diverge from 6 month onward, such that by 12 month the infants of control mothers weighed 8.98 ± 0.62 kg, compared with 9.39 ± 0.66 kg for the treated group. The incremental increase in weight during the 12-month period was 5.92 ± 0.92 kg for the infants of control mothers and 6.39 ± 0.78 kg for the infants of treated mothers. A similar pattern was observed for length, with divergence from 6 month onward and a difference of 1.2 cm at the age of 1 year (76.2 ± 1.9 cm for infants of treated mothers, compared with 74.6 ± 1.7 cm) 13.
Vitamin D supplementation benefited the classic vitamin D function of bone growth, as evidenced by greater length and weight. In conclusion, vitamin D supplementation after birth should be recommended during the first year of life. The findings support the importance of vitamin D supplementation during the first year of life in full term infants who are exclusively breast fed, for its importance for the skeletal system and thus preventing stunting, morbidity and mortality.
Role of contributors: RT- study design, written manuscript, VNK- Concept, guidance and final review,PS-Carried over methodology and followup of patients
Conflicts of interest: Nil
Funding Source and its role in study: None
VitaminD supplementation improved weight, height in exclusively breastfed infants, 3 month onwards. No significants adverse reactions were noted.
References:
1. D Bringhurst FR, Demay MB, Krane SM, Kromenberg HM. Bone and mineral metabolism in health and disease. In: Kasper DL, Fauci AS, Longo DL, Braunwald E, Hauser SL, Jameson JL, eds. Harrison’s principles of internal medicine. 16th ed. New York: McGraw Hill; 2005. p.2238-48.
2. Holick MF. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancer, and cardiovascular disease. Am J Clin Nutr. 2004;80(6):1678S-88S.
3. Marriott BM. Vitamin D supplementation: A word of caution. Ann Int Med. 1997;127 (3):231-3.
4. Norman AW. Sunlight, season, skin pigmentation, vitamin D, and 25-Hydroxy vitamin D: Integral components of the vitamin D endocrine system. Am J Clin Nutr. 1998;67:1108- 10.
5. Compston JE. Vitamin D deficiency: Time for action. BMJ. 1998;317:1466-7.
6. Fraser DR.Vitamin D. Lancet. 1995;345:104- 7.
7. Raiten DJ, Piciano MF. Vitamin D and health in 21st Bone and beyond. Am J Clin Nutr. 2004;80(suppl):1673S- 7S.
8. Holick MF. The vitamin D epidemic and its health consequences.J of Nutr.2005;135: 2739S-2748S.
9. Gropper S, Smith J, Groff J. Advanced Nutrition and Human Metabolism. 4th ed.Belmont, C.A.: Wadesworth Publishing, 2004
10. Victora CG, de Onis M, Hallal PC, Blossner M, Shrimpton R. Worldwide timing of growth faltering: revisiting implications for interventions. Pediatrics. 2010; 125 :e473-80.
11. Geeta TK et al. Effect of weekly vitamin D supplements on mortality, morbidity, and growth of low birthweight term infants in India up to age 6 months: randomised controlled trial. Br Med J 2011;342:2975.
12. El-Mazary, A. A. M., et al. “Vitamin D Supplementation and the Risk of Infections in Full term Infants. Correlations with the Maternal Serum Vitamin D.”Archives of Disease in Childhood 97.Suppl 2 (2012): A257-A257.
13. Brooke, O. G., et al. “Vitamin D supplements in pregnant Asian women: effects on calcium status and fetal growth.” BmJ 280.6216 (1980): 751-754
Issue: January-March 2018 [Volume 7.1]