Clinico-Etiological Profile Of Neonatal Seizures In Term Neonates
Original Research
Original Research
![]()
Abstract:
Background : Neonatal seizures or neonatal convulsions are epileptic fits occurring from birth to the end of the neonatal period. Neonatal seizures are a common neurological problem with a frequency of 1.5-14/1000 neonates. Neonatal seizure is common in this part of the Telangana and there was paucity of data from this area. Identification of etiology will help in management there by reducing morbidity and mortality. Materials and methods: This prospective study was done in NICU of S.V.S. Medical College and Hospital, Mahabubnagar, from Jan 2016 to Jan 2017. Term neonates with clinically identifiable seizure were included in the present study. This study was approved by institutional ethical committee and written consent was obtained from parents of the studied neonates. Results: Of 84 studied neonates, 46 were males and 38 were females. 29 neonates had seizures within first 24 hours and 22 neonates had seizures on day 2. Perinatal asphyxia was seen in 28 neonates and septicemia was seen in 21 neonates.Conclusion: Perinatal asphyxia was the most common cause for neonatal seizures in term neonates, followed by septicaemia and metabolic disturbances.
Key words: Neonatal seizures, perinatal asphyxia, septicaemia.
Introduction:
Neonatal seizures or neonatal convulsions are epileptic fits occurring from birth to the end of the neonatal period1.Neonatal seizures are a common neurological problem with a frequency of 1.5-14/1000 neonates. The seizures in neonates may manifest as paroxysmal alteration in motor, sensory, behavioral or autonomic dysfunctions2. Clinically, there are four seizure types: subtle, clonic, tonic, and myoclonic. Each one can be focal, multifocal, and generalized3. Etiologically, about 80-85% of neonatal seizures are symptomatic and rest are idiopathic. The most common cause is hypoxic–ischemic encephalopathy (HIE); the other causes include hemorrhage, metabolic disturbances, and infections4. Seizures are often the first sign of neurological dysfunction in newborns5. Infants with neonatal seizures are at increased risk of morbidity and mortality. The babies who survive may have adverse effects on motor, cognitive, and behavioraldevelopment or epileptic complications in the later part of the life6.
The present study was conducted to determine the etiological factors for neonatal seizures in our hospital. The result of the study will help in planning management of neonatal seizure to improve the short term as well as long term outcome.
Methods :
This prospective study was done in NICU of S. V. S. Medical College and Hospital, Mahabubnagar, from Jan 2016 to Jan 2017. This study was approved by institutional ethical committee and written consent was obtained from parents of the studied neonates.
All the term neonates with clinically identifiable seizures before 28 days of life were enrolled in the study. Preterm neonates, babies with neonatal tetanus, and babies with obvious congenital malformation were excluded.
A detailed antenatal, natal, postnatal, and family history was obtained and documented in predesigned proforma.Diagnosis of HIE was based on history, physical examination, Apgar score, arterial blood gas, brain MRI brain or cranial sonography. Diagnosis of neonatal infection was based on clinical manifestations, sepsis screening tests and blood culture, CSF analysis.
Metabolic disorders were considered as hypoglycemia(serum glucose<40mg/dl), hypocalcemia (Total serum Ca <8mg/dl in full term.), and hypomagnesaemia (serum magnesium levels < 1.5 mg/Dl). Intracranial hemorrhages were diagnosed by CT scan brain. The results were analyzed by appropriate statistical methods.
Results:
In the present study, 84 neonates with chief complaints of seizures were included. 46 (55%) were males and 38 (45%) were females. 53 (63.1%) neonates were between 37 to 39weeks of gestation, while 31 (36.9%) neonates were between 40 to 41 weeks of gestation. 44 neonates had vaginal delivery and 40 neonates were delivered by cesarean section.
Onset of seizure was day 1 in 29 (34.5%), day 2 in 22 (26.2%), and day 3 of life in 8 (9.5%) neonates. The most common type of seizure seen was focal clonic type (n=28, 33.3%); followed by subtle seizures (n=26, 31%), myoclonic (n=15, 17.9%), focal tonic (n=7, 8.3%), multifocal (n=, 6%), and generalized tonic clonic type (n=3, 3.6%).
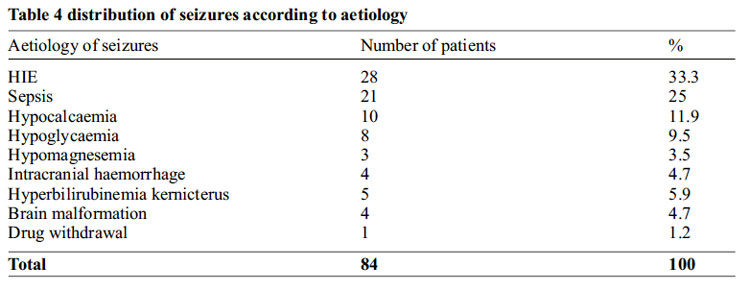
Among the studied population, perinatal asphyxia was identified as the most common cause of neonatal seizure (n=28, 33.3%). This was followed closely by septicemia (n=21, 25.0%).
Other significant causes identified were hypocalcemia (n=10, 11.9%), hypoglycemia (n=8, 9.5%), hyperbilirubinemia (n=5, 6%), intracranial hemorrhage (n=4, 4.7%) brain malformations (n=4, 4.7%. While, 3 (3.5%) neonates had hypomagnesaemia and 1(1.2%) neonate had seizures due to lignocaine injection.
Discussion:
Neonatal seizures are a common neurological problem with a frequency of 1.5- 14/1000 neonates. Etiologically, about 80-85% of neonatal seizures are symptomatic and rest are idiopathic. The most common cause is hypoxic–ischemic encephalopathy (HIE); the other causes include hemorrhage, metabolic disturbances, and infections4.
In our present study, 46 (54.76%)neonates were male and 38 (45.23%) were females with slight male predominance 1.2:1 (Table No 6 and Graph No 2) table no 1. This finding was similar to the studies done by the Sahana G et al7, Sabzehei MK et al3, Parvin R et al8 andMoayedi A.R et al9.
44 (52%)babies with neonatal seizure were born through the vaginal delivery and 40 (47%) babies were through the LSCS. This was found similar with the study done by Sabzehei MK et al3(53% and 47% respectively).
Of the 84 neonates with seizures, 29 (34.5%) had seizures on day 1 followed by 22 (26.2%) on day 2 of life, 8 (9.5%) on day 3, and 10 (11.9%) on day >=8 days of life. A total of 59 (50.3%) neonates had seizures within first 3 days of life (table 2). Similar findings was found by the Sahana G et al7 and Ronen Gabriel et al10.
Based on clinical seizure types, 28 (33.3%) neonates had focal clonic type followed immediately by the subtle seizures in 26 (31.0%). Myoclonic type of seizures was seen in 15 (17.9%), focal tonic type in 7 (8.3%) and multifocal type in 5 (6. 0%) neonates.This was found in concordance with the study done by Aziz A Et al11 and Verma YS et al12. (Table No 9 and Graph No 5). Table no 3
Perinatal asphyxia was the most common cause of neonatal seizures identified in 33.3% of neonates. (Table no 15). This was found to be in concordance with the study done by NajeebS et al13 (46%) Sabzehei MK et al3 (34%), Glass HC et al14 (38%) and Malik BA et al15 (35%). In other studies, done by Verma YS et al12 (70%) of neonates had seizures due to hypoxic ischemic encephalopathy.
In the present study 21(25%) of 84 babies had sepsis (septicemia and meningitis). This was found similar to the study done by Parvin R et al8 (26%, n=51), Sabzehei MK et al3(24.4% n=102) and was found to be (29%) by the study done by NajeebS et al13. In another study done by Malik BA et al15 34% of babies had septicemia. In the present study 1(4.8%) baby had herpes infection as the cause for seizure which was found similar to the study done by Parvin R et al8 (1.96%)
Seizures due to hypoglycemia in association with comorbidities like HIE, Septicemia and IDM were accounted for 37 (44%) whereas 8 (9.5%) babies had seizure only due to hypoglycemia without any comorbidities. This was seen in concordance with the study done byKumar A et al5 (11.11%), Sahana G et al7 (9.17%). This is probably because of depletion of glycogen storage and inadequate feeding during early post-natal days.
Seizures due to hypocalcemia associated with other comorbidities like perinatal asphyxia, septicemia and IDM were 19(22.6%) babies, whereas isolated hypocalcemiacausing seizures were found in 10 (11.9%) of the 84 neonates studied. This was found similar to the study done by Parvin R et al815.65% (n=51) and Taksande A M et al16 (n=110) where they found to be 11.8% and Verma YS et al12 found it to be 11.67% (n=60). In 3 (3.5%) cases neonatal seizure was caused by hypomagnesemia. Similar finding was seen by Taksande A. M et al16.
Seizures due to hyperbilirubinemia (kernicterus) was seen in 5 (6%) neonates in the present study. Similar findings were found in study done by NajeebS et al13 (n=6, 6%). 4 (4.7%) neonates had seizures due to intracranial hemorrhage. Similar findings were seen by NajeebS etal13 (n=100, 4%) and SudiaS et al17 (n=90, 4.6%). Seizures due to lignocaine toxicity was seen in 1 (1.2%) neonate in our study, similar finding was seen by Malik BA et al15 (n=2, 1%).
Conclusion:
The present shows perinatal asphyxia is the most common cause of neonatal seizures among term neonates in our setup. The other causes followed in order are septicemia, metabolic (hypoglycemia, hypocalcemia, hypomagnesemia and hyperbilirubinemia), intracranial hemorrhages and brain malformations. Early identification of at risk pregnancies, institutional delivery and aseptic precautions with timely resuscitation is recommended to reduce morbidity and mortality due to neonatal seizures.
Declarations: Funding: None
Conflict of interest: None
Ethical approval: Approved by hospital ethical committee
References:
1. Panayiotopoulos CP. The Epilepsies: Seizures, Syndromes and Management. Oxfordshire (UK) : Bladon Medical Publishing; 2005. Chapter 5, Neonatal Seizures and Neonatal Syndromes. Available from: https://www.ncbi. nlm.nih. gov /books /NBK2599/
2. Das D, Debbarma S. A Study on Clinico- Biochemical Profile of Neonatal Seizure. Journal of Neurology Research, North America, 6, dec. 2016. Available at: <http://www.neurores.org/index.php/neurore s/article/view/404/399>. Date accessed: 20 May. 2017.
3. Sabzehei MK, Basiri B, Bazmamoun H. The Etiology, Clinical Type, and Short Outcome of Seizures in Newborns Hospitalized in Besat Hospital/Hamadan/ Iran. Iran J Child Neurol. 2014 Spring;8(2):24-8.
4. Kang SK, Kadam SD. Neonatal Seizures: Impact on Neurodevelopmental Outcomes. Front Pediatr. 2015 Nov 23;3: 101. doi: 10.3389/fped.2015.00101. eCollection 2015.
5. Kumar A, Gupta A, Talukdar B. Clinicoetiological and EEG profile of neonatal seizures. Indian J Pediatr.2007 Jan;74(1):33-7.
6. M Levene. The clinical conundrum of neonatal seizures. Arch Dis Child Fetal Neonatal Ed. Mar 2002; 86(2): F75–F77. doi: 10.1136/fn.86.2. F75.
7. Sahana G, Anjaiah B. Clinical profile of neonatal seizures. International journal of medical and applied sciences. Jan-March. 2014, Volume 3 Issue 1 page 21-27.
8. Parvin R, Afmsalim, Rahman M, Chowdhury K, Sultana A, Ahmed S, et al. Neonatal Seizures: Correlation between Clinico- Etiological Profile and EEG Findings. Bangladesh J Child Health 2014; Vol 38 (1): 19-23.
9. Moayedi, AR; Zakeri, S.; Moayedi, F. Neonatal seizure: etiology and type. Iranian Journal of Child Neurology, [S.l.], v. 2, n. 2, p. 23-26, nov. 2008. ISSN 2008-0700. Available at: <http://journals.sbmu.ac.ir/index.php/ ijcn/article/view/458>. Date accessed: 17 Dec. 2014.
10. Ronen GM, Rosales TO, Connolly M, A n d e r s o n V E , L e p p e r t M . S e i z u r e characteristics in chromosome 20 benign familial neonatal convulsions. Neurology. 1993 Jul; 43(7):1355-60.
11. Aziz A, Gattoo I, Aziz M, Rasool G. Clinical and etiological profile of neonatal seizures: a tertiary care hospital based study. Int J Res Med Sci. 2015; 3:2198-2203.
12. Verma YS, Dutt R, Rajput N, Patil R. Predictive value of EEG for neurodevelopmental outcome in neonatal seizures”. Journal of Evolution of Medical and Dental Sciences 2013; Vol2, Issue 29, July 22; Page: 5417- 5425.
13. Najeeb S, Qureshi AM, Anis-ur-Rehman, Ahmad F, Shah S, Khan AY, et al. Aetiology and types of neonatal seizures presenting at Ayub Teaching Hospital Abbottabad. J Ayub Med Coll Abbottabad. 2012 Jan-Mar; 24(1):33-7.
14. Glass HC, Shellhaas RA, Wusthoff CJ, Chang T, Abend NS, Chu CJ. Et al. Contemporary Profile of Seizures in Neonates: A Prospective Cohort Study. J Pediatr. 2016 Jul; 174:98- 103.e1. doi: 10.1016/j.jpeds.2016.03.035. Epub 2016 Apr 19.
15. Malik BA, Butt MA, Shamoon M, Tehseen Z, Fatima A, Hashmat N. Seizures etiology in the newborn period. J Coll Physicians Surg Pak. 2005 Dec; 15(12):786-90.
16. Taksande AM, Krishna V, Manish Jain, Mahaveer L. Clinico-biochemical profile of neonatal seizures. PaedOncall Journal 2005 October; 2(10). Available from: http://www.pediatriconcall.com/Journal/Arti cle/FullText.aspx?artid=737&type=J&tid=&i mgid=&reportid=326&tbltype=
17. Sudia S, Berwal PK, Nagaraj N, Jeavaji P, Swami S, Berwal A. Clinicoetiologicalprofile and outcome of neonatal seizures. Int J ContempPediatr 2015;2:389-90

Issue: July-September 2017 [Volume 6.3]