Association of Modifiable maternal risk factors with congenital heart diseases in children – a case-control study
Original Research
Original Research
![]()
Abstract:
Background: Congenital Heart diseases (CHD) are among the most common congenital malformations and are the leading cause of neonatal and infant mortality. Emerging data suggests that there are maternal risk factors which can increase the occurrence of CHD in the baby, many of which are potentially modifiable. Hence knowledge of those risk factors provides an opportunity to prevent CHD with appropriate intervention. This study was undertaken to contribute to the existing understanding by finding the correlation between various modifiable maternal risk factors and CHD in the offspring. Setting and Design- This was 1:2 matched casecontrol study, conducted in the Department of Pediatrics, MGIMS Sevagram, a teaching rural based hospital in Central India, from November 2010 to May 2012 Materials and Methods- 200 cases of CHD diagnosed on echocardiography and 400 age and sex matched controls were enrolled in the study. The history regarding various maternal risk factors was enquired using the same questionnaire for both cases and controls. Statistical Analysis-The analysis was done using EPI 6 software, univariate and multivariate logistic regression model were used to establish the statistical significance of the association between risk factors and CHD. The association was considered statistically significant when OR>1. Results : Maternal history of fever, tobacco chewing, antenatal drugs exposure, bad obstetric history and pregestational diabetes mellitus were found to be significantly associated with higher risk of CHD in the baby.Conclusion- This study was aimed at improving the knowledge related to risk factors associated with CHD in a rural Indian scenario. The information can be utilized for prevention of CHD by a well-structured approach to identify and guide the prospective parents that could reduce the likelihood that their child will have a major cardiac malformation by the control of associated risk factor.
Introduction :
Congenital Heart Disease (CHD) is a gross structural abnormality of the heart or intrathoracic great vessels that is actually or potentially of functional significance. It is the most common congenital problem that accounts for up to 25% of all congenital malformations that present in the neonatal period and is leading cause of neonatal and infant mortality .The burden of CHD in India is likely to be enormous due to very high birth rate and its prevalence varies from 2.25-5.2 per 1000 population in different parts of India .
There are modifiable and nonmodifiable risk factors of CHD. The modifiable risk factors include maternal illnesses like diabetes, antenatal therapeutic drug exposure e.g. anticonvulsants and nontherapeutic drug exposures e.g. alcohol, antenatal infections like influenza, antenatal radiation exposure, maternal stress and smoking, and environmental exposures like organic solvents. Nonmodifiable risk factors include advanced maternal and paternal age, maternal illnesses like phenylketonurea, SLE etc, race, ethnicity, reproductive history.(3)
The heavy burden of CHD emphasizes the importance of this group of heart diseases. Over the past decade, there have been major breakthroughs in the understanding of inherited causes of congenital heart disease, including the identification of specific genetic abnormalities for some types of malformations but there is relatively less information on noninherited modifiable factors that may have an adverse effect on the fetal heart. Prevention of CHD has been hampered by a lack of information about modifiable risk factors for abnormalities in cardiac development, Hence this study was aimed at improving the knowledge related to modifiable risk factors associated with CHD in a rural Indian scenario.
Material And Methods:
This was a case-control study conducted in the Department of Pediatrics of Mahatma Gandhi Institute of Medical Sciences, Sevagram, which is a teaching hospital in rural central India.After approval from the ethics committee of the institute, this study was conducted from November 2010 to May 2012.
Cases and controls were taken from the children who were admitted or visited OPD during the study period. Informed consent was taken from all the study subjects, those who did not give consent were excluded. Children with age<3yrs with clinical features suggestive of CHD were further evaluated and the diagnosis was confirmed with echocardiographic examination. Those with confirmed CHD diagnosis were included as cases (n=200) and age and sex matched children without CHD were taken as controls(n=400). Parents of all the subjects (cases as well as controls) were interviewed using study questionnaire in a similar manner during the study period and history of various maternal risk factors (h/o previous still births/ spontaneous abortions and exposures to infection, medication, fever and radiations, maternal age at pregnancy, history of diabetes in mother and addiction to smoking, tobacco chewing and alcohol) were enquired. Statistical analysis was done with EPI 6 software using univariate and multivariate model and strength of association was established by calculating OR.
Results:
The mean age of cases and controls was 15.7+13.04 months. In the study cohort, 52.5% were males and 47.5% were females. Out of total 200 cases of CHD, 163 had acyanotic Heart disease(81.5%) and 37 had cyanotic heart disease (18.5%).The most common congenital heart disease was Ventricular Septal Defect( VSD )and was found as an isolated lesion in 64 patients which constituted 32% of total CHD followed by Patent Ductus Arterisos (PDA), Atrial Septal Defect (ASD) and Tetralogy Of Fallot(TOF). On univariate analysis history of maternal age>35yrs at the time of pregnancy, maternal h/o fever during pregnancy, exposure to tobacco chewing during pregnancy,maternal drug exposure in form of valproic acid, phenytoin, bad obstetric history, maternal pregestational diabetes mellitus, were found to be statistically significant. Table 1.
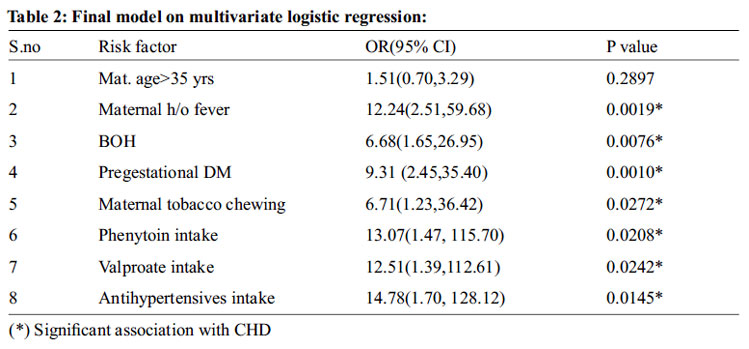
The independent variables which were found to be significant on univariate analysis were pushed into the multivariate model to control for the confounding variables. On multivariate logistic regression analysis advanced age during pregnancy lost its significance. A significant association was found with following maternal antenatal risk factors i.e. maternal fever, tobacco chewing, and antenatal drugs exposure, bad obstetric history, pregestational diabetes mellitus as shown in table 2.
Discussion:
This study was conducted to determine the association of modifiable maternal risk factors with CHD. We have found that maternal fever during pregnancy, tobacco chewing, antenatal drugs exposure (phenytoin & valproate), bad obstetric history, antihypertensive drug use(ACE inhibitors & beta blockers), pregestational diabetes mellitus were associated with increased risk of CHD in the baby. However following risk factors were not found to be significantly associated with CHD i.e. antenatal radiation exposure, antenatal use of NSAIDs, alcohol consumption and smoking, gestational diabetes and maternal age >35 years at the time of pregnancy.
We found no association between advanced maternal age and occurrence of CHD, OR:1.3 (95%CI:0.58-3.03), this was similar to those observed by Shiwei Liu et al (4) but it was in contrast to Reefhuis et al(5) and Miller et al (6) who observed significant association between advanced maternal age and CHD. Significant association was observed between history of fever in first trimester of pregnancy and occurrence of CHD in the offspring [OR 12.24(95% CI-2.51,59.68)] these were similar to those observed by Tikkannen et al(7) ,Botto et al(8) and Shiwei Liu et al (4) .It is well known that maternal rubella causes congenital malformations in the offspring but in our study, we found no association between rubella infection and CHD OR: 6.05(95% CI- 0.64, 160.33), these contrary findings could be due to low prevalence of rubella in this region.
We found no statistically significant association between antenatal alcohol consumption and occurrence of CHD [OR- 6.05 (95%CI-0.64-160.33)]. These results were in contrast to other studies like Mateja et al (9) who observed the increase in congenital heart defects in babies born to mothers who reported binge drinking. Carmichael et al (10) observed that relative to nonconsumers, women who consumed alcohol less than once a week had a 1.3-fold increased risk of delivering infants with a conotruncal heart defect, and women who consumed alcohol once a week or more had a 1.9- fold increased risk. Pejtsik et al (11) found a significant association between alcohol consumption and occurrence of cardiac defects in offspring.Association was also not observed between maternal tobacco smoking and occurrence of CHD with the history of smoking during pregnancy present in only 1 % of mothers, OR: 2.00 (95% CI: 0.20-19.40). Malik et al (12) concluded stronger association for septal defects in infants exposed to medium (15-24 cigarettes/day) and heavy smoking (>25cigarettes/day) compared with light smoking (1-14 cigarettes/day) exposure. Chehab et al (13) found pulmonary stenosis was highly associated with mothers who smoked 20 cigarettes or more per day.
Contrary to all the above studies, in our study, we did not find any significant association between alcoholism and smoking in mother and occurrence of cardiovascular defects in the baby, probably due to the low prevalence of alcoholism and smoking in females in this area. On the other hand, tobacco chewing is highly prevalent in this area and significant association was observed between maternal consumption of smokeless tobacco during pregnancy and occurrence of CHD with OR: 6.71(95% CI: 1.23, 36.42)
We found a significant association between maternal pregestational diabetes mellitus and occurrence of CHD in the offspring OR-9.31(95% CI:2.45-35.40). These findings were in accordance to those observed by Becerra et al (14) , Wren et al (15), Loffredo et al (16) and Frencz et al (17).A significant association was not observed between Gestational diabetes mellitus and occurrence of CHD with OR-2.00(95% CI:0.20-19.40). Antihypertensive drug (ACE inhibitors and beta blockers) intake during pregnancy was found in 3% of the mothers and we found statistically significant association between antenatal antihypertensive drugs exposure and CHD with OR:14.78(95% CI:1.70-128.12) Similar results were obtained in studies by Lennestal et al (18) and De Kun Li et al(19). We found significant association between valproate consumption during early pregnancy and occurrence of congenital heart disease in the offspring with OR 12.51(95%CI- 1.39, 112.61) which was consistent with the finding of Jentink J et al(20) Samren et al(21) and Vajda et al(22).
We also found significant association between maternal intake of phenytoin monotherapy during pregnancy and occurrence of CHD with OR: 13.07(95%CI: 1.47-115.70). This was similar to a study by Herandez et al . In our study, we found no significant association between maternal intake of NSAIDs during pregnancy and occurrence of CHD with OR: 2.00;( 95% CI: 0.20- 19.40). These results were similarto those observed by Cleves MA et al andNeilsen et al . On the contrary study by Ofori et al , significant association was observed between septal closure defect and intake of NSAIDs during pregnancy.
No statistically significant association was found between radiation exposure and occurrence of CHD this was similar to finding by Zang et al and Roman et al .Contrary to the finding of above 2 studies, a case-control study by Matte et al on health care workers, observed significant association between radiation exposure during pregnancy and occurrence of coarctation of aorta in the offspring.
Past history of still births/spontaneous abortions was significantly associated with occurrence of CHD in the offspring with OR-6.68 (95%CI:1.65-26.95) , these findings were in accordance with Baltimore Washington Infant study(30) which concluded that history of reproductive problems has been associated with an increased risk of tetralogy of Fallot (previous miscarriage, nonchromosomal atrioventricular septal defects (previous stillbirth, ASDs (previous preterm birth) and Ebstein’s anomaly (previous miscarriage). In the study by Shiwei Liu et al , similar finding was observed on univariate logistic analysis OR-3.06 (95%CI-1.19–7.87) but on multiple regressions controlling for confounding factors they did not found significant association between previous history of spontaneous abortion and occurrence of CHD in the offspring.
Since the study was conducted in a rural tertiary care hospital, so the finding of the study cannot be generalized to the population as a whole. This is the inherent limitation of a hospital-based study compared to community-based study. Thesubjects included were only 200 cases and 400 controls, had it been a larger number the results would have been more significantly generalized to the population as a whole.
Conclusion:
Congenital Heart Disease is a leading cause of infant and neonatal mortality and various modifiable and nonmodifiable risk factors result in development of CHD in the foetus. Understanding modifiable risk factors associated with CHD is crucial so that morbidity and mortality due to CHD could be reduced by giving appropriate advice to the parents and guideline could be framed for the prevention of CHD by decreasing the modifiable risk factors.The risk approach should be implemented with all seriousness to detect and offer special care to high-risk mothers in our resource-limitedscenario. As there is a paucity of data related to the risk factors associated with congenital heart disease in rural Indian scenario, this study can serve as a baseline data to compare and follow for further studies.
Funding: None Financial disclosure: The authors have indicated they have no financial relationships relevant to this article to disclose. Conflict of interest: The authors have no conflicts of interest relevant to this article to disclose
References:
1. Mitchell SC, Korones SB, Berendes HW. Congenital heart disease in 56,109 births. Incidence and natural history. Circulation. 1971;43(3):323-32. 3.
2. Saxena A. Congenital heart disease in India: a status report. Indian journal of pediatrics. 2005;72(7):595-8. Epub 2005/08/04.
3. Jenkins KJ, Correa A, Feinstein JA, Botto L, Britt AE, Daniels SR, et al. Noninherited risk factors and congenital cardiovascular defects: current knowledge: a scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young: endorsed by the American Academy of Pediatrics. Circulation. 2007;115(23):2995- 3014. Epub 2007/05/24.
4. Liu S, Liu J, Tang J, Ji J, Chen J, Liu C. Environmental risk factors for congenital heart disease in the Shandong Peninsula, China: a hospital-based case-control study. Journal of epidemiology / Japan Epidemiological Association. 2009;19(3): 122-30. Epub 2009/04/29.
5. Reefhuis J, Honein MA. Maternal age and non-chromosomal birth defects, Atlanta– 1968-2000: teenager or thirty-something, who is at risk? Birth defects research Part A, Clinical and molecular teratology. 2004;70(9) : 572-9. Epub 2004/09/16.
6. Miller A, Riehle-Colarusso T, Siffel C, Frias JL, Correa A. Maternal age and prevalence of isolated congenital heart defects in an urban area of the United States.
7. American journal of medical genetics Part A. 2011;155A(9):2137-45. Epub 2011/08/05. 7. Tikkanen J, Heinonen OP. Maternal hyperthermia during pregnancy and cardiova-scular malformations in the offspring. European journal of epidemiology. 1991;7(6): 628-35. Epub 1991/11/01.
8. Botto LD, Lynberg MC, Erickson JD. Congenital heart defects, maternal febrile illness, and multivitamin use: a populationbased study. Epidemiology. 2001;12(5):485- 90. Epub 2001/08/16.
9. Mateja WA, Nelson DB, Kroelinger CD, Ruzek S, Segal J. The association between maternal alcohol use and smoking in early pregnancy and congenital cardiac defects. J Womens Health (Larchmt). 2012;21(1):26- 34. Epub 2011/09/08.
10. Carmichael SL, Shaw GM, Yang W, Lammer EJ. Maternal periconceptional alcohol consumption and risk for conotruncal heart defects. Birth defects research Part A, Clinical and molecular teratology. 2003;67(10):875-8. Epub 2004/01/28.
11. Pejtsik B, Pinter J, Horvath M, Hadnagy J. [Relationship between congenital heart disease & various factors affecting pregnancy]. Orvosi hetilap. 1992;133(3):155-8. Epub 1992/01/19.
12. Malik S, Cleves MA, Honein MA, Romitti PA, Botto LD, Yang S, et al. Maternal smoking and congenital heart defects. Pediatrics. 2008;121 (4):e810-6.
13. Chehab G, El-Rassi I, Adhami A, Chokor I, Chatila F, Haddad W, et al. [Parental smoking during early pregnancy and congenital heart defects]. Le Journal medical libanais The Lebanese medical journal. 2012;60(1):14-8. Epub 2012/06/01. Tabagisme parental en debut de grossesse et cardio- pathies congenitales.
14. Becerra JE, Khoury MJ, Cordero JF, Erickson JD. Diabetes mellitus during pregnancy and the risks for specific birth defects: a population -based case-control study. Pediatrics. 1990;85 (1): 1-9. Epub 1990/01/01.
15. Wren C, Birrell G, Hawthorne G. Cardiovascular malformations in infants of diabetic mothers. Heart.2003;89(10):1217- 20. Epub 2003/09/17.
16. Loffredo CA, Wilson PD, Ferencz C. Maternal diabetes: an independent risk factor for major cardiovascular malformations with increased mortality of affected infants. Teratology. 2001;64(2):98-106. Epub 2001/07/19.
17. Ferencz C, Rubin JD, McCarter RJ, Clark EB. Maternal diabetes and cardiovascular malformations: predominance of double outlet right ventricle and truncus arteriosus. Teratology. 1990;41(3):319-26.
18. Lennestal R, Otterblad Olausson P, Kallen B. Maternal use of antihypertensive drugs in early pregnancy and delivery outcome, notably the presence of congenital heart defects in the infants. European journal of clinical pharmacology. 2009;65(6):615-25.
19. Li DK, Yang C, Andrade S, Tavares V, Ferber JR. Maternal exposure to angiotensin converting enzyme inhibitors in the first trimester and risk of malformations in offspring: a retrospective cohort study. BMJ. 2011;343:d5931.
20. Jentink J, Loane MA, Dolk H, Barisic I, Garne E, Morris JK, et al. Valproic acid monotherapy in pregnancy and major congenital malformations. The New England journal of medicine. 2010;362(23):2185-93.
21. Samren EB, Van Duijn CM,Koch S,Hiilesmaa VK,Klepel H,BardyAH, Mannagetta GB. Maternal use of Antiepileptic Drugs and the Risk of Major Congenital malformations: A Joint European Prospective Study of Human Teratogenesis Associated with Maternal Epilepsy. Epilepsia. 1997;38(No 9).
22. Vajda FJ, Hitchcock A, Graham J, Solinas C, O’Brien TJ, Lander CM, et al. Foetal malformations and seizure control: 52 months data of the Australian Pregnancy Registry. European journal of neurology: the official journal of the European Federation of Neurological Societies. 2006;13(6):645-54. Epub 2006/06/27.
23. Hernandez-Diaz S, Werler MM, Walker AM, Mitchell AA. Folic acid antagonists during pregnancy and the risk of birth defects. The New England journal of medicine. 2000;343(22):1608-14. Epub 2000/11/30.
24. Cleves MA, Savell VH, Jr., Raj S, Zhao W, Correa A, Werler MM, et al. Maternal use of acetaminophen and nonsteroidal antiinflammatory drugs (NSAIDs), and muscular ventricular septal defects. Birth defects research Part A, Clinical and molecular teratology. 2004;70(3):107-13. Epub 2004/03/25.
25. Nielsen GL, Sorensen HT, Larsen H, Pedersen L. Risk of adverse birth outcome and miscarriage in pregnant users of non-steroidal anti-inflammatory drugs: population based observational study and case-control study. BMJ. 2001;322(7281):266-70. Epub 2001/02/07.
26. Ofori B, Oraichi D, Blais L, Rey E, Berard A. Risk of congenital anomalies in pregnant users of non-steroidal anti-inflammatory drugs: A nested case-control study. Birth defects research Part B, Developmental and reproductive toxicology. 2006;77(4):268-79. Epub 2006/08/25.
27. Zhang J, Cai WW, Lee DJ. Occupational hazards and pregnancy outcomes. American journal of industrial medicine. 1992;21(3):397-408. Epub 1992/01/01.
28. Roman E, Doyle P, Ansell P, Bull D, Beral V. Health of children born to medical radiographers. Occupational and environmental medicine. 1996;53(2):73-9. Epub 1996/02/01.
29. Matte TD, Mulinare J, Erickson JD. Casecontrol study of congenital defects and parental employment in health care. American journal of industrial medicine. 1993;24(1):11- 23. Epub 1993/07/01.
30. Jenkins KJ, Correa A, Feinstein JA, Botto L, Britt AE, Daniels SR, et al. Noninherited risk factors and congenital cardiovascular defects: current knowledge: a scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young: endorsed by the American Academy of Pediatrics. Circulation. 2007;115(23):2995- 3014. Epub 2007/05/24.

Issue: July-September 2017 [Volume 6.3]