Estimation of Zinc Levels in Children with Acute Lower Respiratory Tract Infection: A Case Control Study
Original Research
Corresponding Author: Dr. Sachin Damke, Professor, Department of Pediatrics, Jawaharlal Nehru Medical College and Acharya Vinoba Bhave Rural Hospital, Sawangi (Meghe), Wardha.
E-mail id: buntydamke@gmail.com Phone no: (+91)9423727318, (+91)9323234457
Received: 3rd March, 2019 Reviewed: 8th June, 2019, Accepted: 25th June, 2019.
Citation of article: Shreyas Rajendra Borkar, Sachin Damke, Revat Meshram. Estimation of Zinc Levels in Children with Acute Lower Respiratory Tract Infection: A Case Control Study. New Indian Journal of Pediatrics, 2019;8.2.
Original Research
![]()
Abstract: Background: Establishment of zinc’s role in treating illnesses in children has catapulted a greater involvement of researchers, especially for illnesses like acute lower respiratory tract infection (ALRTI). Thus, this study was under taken to estimate serum zinc levels in cases of ALRTI and also correlate it with clinical course of ALRTI.
Materials and Methods: It was a hospital based case-control study involving 61 cases aged 2 months to 5 years with ALRTI and age, sex and nutritionally matched controls. Serum zinc level was estimated at admission. Detailed history, socio-demographic details and examination were noted along with details of clinical course like duration of stay, oxygen requirements, severity of disease and outcome.
Results: The mean serum zinc level of cases was found to be significantly lower than that of controls (Cases 58.88 ± 12.40 ug/dl, Controls 85.36 ± 16.27 ug/dl)(p value = 0.0001).There was a negative correlation of zinc levels with duration of stay (r = -0.052)(p value = 0.691). The mean serum zinc levels were significantly lower in cases of severe pneumonia as compared to cases of pneumonia (WHO IMNCI grading) (p value = 0.0001).The mean serum zinc levels were also significantly lower in those requiring higher O2 concentration(p value = 0.0001)and those who died as compared to the discharged patients(p value = 0.0001).
Conclusion: Lower serum zinc levels are significantly associated with ALRTI and the lower the serum zinc levels; the more is the severity of disease and duration of stay in hospital for the patient, along with increased oxygen requirement and also increased incidence of mortality.
Keywords: Serum zinc estimation, acute lower respiratory tract infection, Children, Pneumonia.
Introduction: Globally, acute lower respiratory tract infections or ALRTI, continue to be a persistent and a pervasive health problem, especially in the form of childhood pneumonia. Though its burden has decreased significantly in the developed countries, the developing countries like India are still under its wrath, causing around 125,333 deaths in the postnatal age group of children under 5 years of age in the year 2016. This amounted to 28% of all the deaths in this age group [1].
Malnutrition has often been thought as one of the most important risk factors leading to acquiring infections like ALRTI [2]. With the problem of macronutrient deficiency decreasing significantly, it is the micronutrient deficiency with trace elements like Zinc in particular, which have been implicated and studied recently, for increased susceptibility of children to ALRTI.
Zinc has been linked to the function of more than 300 distinct enzymes responsible for a wide array of functions like synthesis of nucleic acid, proteins, hormones, their receptors and certain immunoregulatory molecules as well as pathways [3].
Zinc also has been demonstrated to have an innate antiviral activity due its role in the production of Interferon [4].
Research across the globe has clearly established the role of Zinc in treatment as well as decreasing severity and susceptibility to diarrhoea in children, but the research regarding its role in treatment as well as decreasing susceptibility to Acute lower respiratory tract infections(ALRTI) has given inconsistent results. Also, there is paucity of studies regarding association of Zinc with the clinical course of ALRTI.
Thus in order to better assess the role of Zinc in ALRTI, this study was undertaken with the aim of quantifying the Zinc levels in the population not suffering ALRTI and comparing it with the population suffering with ALRTI as a Case-Control Study, along with further evaluation of the association of Zinc levels with the clinical course of ALRTI.
Methods:
It was a Hospital based Case-Control Study that was conducted in Department of Pediatrics, Acharya Vinobha Bhave Rural Hospital, Sawangi (Meghe), Wardha. The study was initiated after taking permission from institutional ethics committee. Participants of the study were enrolled after getting an informed consent.
Children between the age of 2 months to 5 years, admitted from the OPD or casualty for Acute Lower Respiratory Tract infection during study period were considered for enrolment as cases. Children suffering from Acute Gastroenteritis or diarrheal illness prior to or during enrolment in the study, or with clinical diagnosis of Reactive airway disease/asthma or with underlying chronic illnesses and congenital heart disease or on zinc supplementation within 1 month prior to enrolment in the study were excluded.
Age, sex and nutritionally matched patients admitted from OPD or casualty for indications other than inclusion and exclusion criteria were enrolled as Controls. Age of the controls was matched within 6 months. The Sample Size was statistically calculated as 61 with the Alpha error being 0.5% and Power being 80% in this two sided study. Thus a total of 61 cases and 61 controls were enrolled in the study.
The detailed demographic information, history, clinical findings, laboratory findings and details of clinical course of cases and controls included in the study were entered in predesigned and validated proforma. Socio-economic status [SES] was assessed according to the Modified Kuppuswamy scale updated in 2017[5].
Detailed General examination was carried out in the patients along with Respiratory system and other systemic examination and a clinical diagnosis was made and entered into the proforma. The details of blood investigations and imaging for confirmation of clinical diagnosis were also noted during the stay of the patient in the hospital.
The serum zinc estimation was done by using colorimetric test. The kit used for this study was manufactured by Centromic GMBH, Germany. The Sample used was serum obtained by centrifugation of 2 ml of blood sample collected at 3000 rpm for 3 to 5 minutes. The blood sample was obtained at Day 1 of admission of cases and controls. In two different ependoff tubes, 1000 ul of reagent in both along with 50 ul of serum in one tube and standard solution in other were mixed and incubated at 37 degree Celsius for 5 minutes. Absorption of the standard A (Standard) and the sample A (Sample) was measured against the reagent blank A (Blank) via the spectrophotometer at 560nm wavelength, which was directly proportional to the concentration of total zinc in the sample [6].
Apart from measuring the serum zinc levels, the details of clinical course of the cases were also documented in terms of the duration of stay, oxygen requirements, severity of disease according to WHO IMNCI grading 2014 and outcome of the cases.
The data obtained from the cases and controls was compiled and entered into Microsoft Excel case sheet. Statistical analysis was done by using descriptive and inferential statistics using chi square test, student’s unpaired t test, one way ANOVA and Pearson’s correlation coefficient and software used in the analysis were SPSS 22.0 version and Graph Pad Prism 6.0 version and p<0.05 was considered as level of significance.
Results: The mean age of cases was 1.55±1.29 yrs and that of controls was 1.95±1.63 yrs.The Sex wise distribution of the cases and controls consisted of 36(59.02%) of cases being male and 25(40.98%) being female as compared to 35(57.38%) of controls being male and 26(42.62%) being female. On comparison, the distribution of cases and controls in this study according to age, sex, nutritional status and socioeconomic status was statistically not significant.
The Mean serum zinc levels in the cases and controls, after comparison, were found to be significantly different [p=0.0001], with mean value for the cases being 58.88 ± 12.40 ug/dl as compared to 85.36 ± 16.27 ug/dl for the controls (Table 1).A total of 33 cases and controls (27.05%) were found to have deficiency of zinc, of which majority (93.93%) were cases (normal range of 60 to 150 ug/dl) [7]
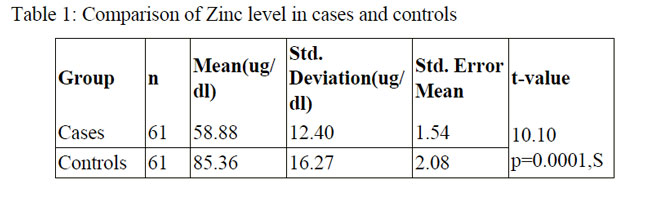
Table 2 shows comparison of serum zinc levels according to the clinical characteristics of cases. Here, the difference in mean serum zinc levels of cases according to WHO IMNCI grading was statistically significant (p value = 0.0001) with cases belonging to Severe Pneumonia group (Mean = 42.88 ± 5.93 ug/dl) having significantly lower value than that of Pneumonia group (Mean = 65.06 ± 7.81 ug/dl).
This is also reflected when we see serum zinc levels according to oxygen requirements, with cases managed on room air having mean of 66.03 ± 7.69 ug/dl, cases requiring supplemental oxygen by nasal prongs having mean of 59.63 ± 10.00 ug/dl and cases requiring mechanical ventilation having mean of 41.41 ± 6.93 ug/dl(Table 2).
The serum zinc analysis of patients according to outcome shows significantly lower zinc values (p value = 0.0001) in cases who eventually died due to the ALRTI and its complications (n = 9) as compared to those who got discharged after treatment (n=52)(Table 2).

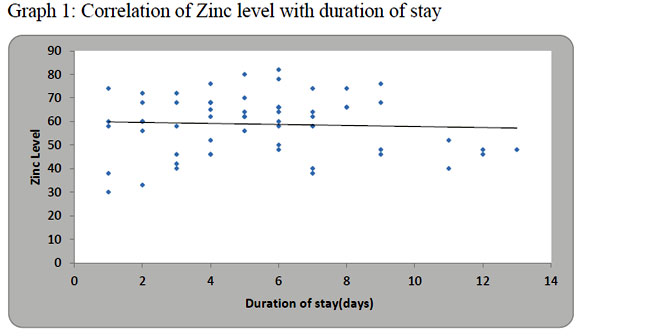
Graph 1 shows the correlation of zinc level with the duration of stay. The mean serum zinc level was found to have a negative correlation (‘r’ = -0.052) with the duration of stay of cases, however, this correlation was statistically not significant (p value = 0.691)
Discussion: The mean serum zinc levels were comparable to that found in the study by Hussain et al.[8].A study in Bangladesh by Shakur et al.and a study in Egypt by Rady et al. showed mean serum zinc levels in cases to be higher than this study [9][10]. On the other hand, a study done by Ibraheem et al. in Nigeria showed mean serum zinc levels of cases to be lower than this study[4]. This variation of mean zinc values can be ascribed to the dietary habits of the country and nutritional status of the subjects of the study as a whole [4] [9] [10].
The difference in serum zinc levels of the cases and controls in this study, as well as in the above mentioned studies is statistically significant (p value = 0.0001). Study by Kumar et al. in India and Arica et al in Greece also showed similar results [11][12]. These finding could be explained by the fact that serum zinc level is decreased by interleukins and tumour necrosis factor α as a part of acute phase reaction in response to inflammatory stimulus [11]
According to disease severity on the basis of WHO IMNCI grading 2014, cases belonging to Severe pneumonia group had significantly lower value than that of pneumonia group and similar findings were seen in study by Rady et al., Hussain et al. and Brooks et.al[8][10][13]. This may be due to the fact that in zinc deficiency, there is loss of immunomodulatory effect of zinc causing unregulated immune response in the respiratory tract, leading to increased airway injury [13].However, evidence to the contrary was found in studies by Bose et al. and Valentiner – Branth et al. [14] [15]. Argument has been put by the above studies that as zinc is required to mount a better immune response by the host against infection, there will be increased damage to the respiratory epithelium due to the increased immune response and thus leading to worsening of symptoms [15].
Regarding the duration of stay of cases, Basnet et al. also found lower duration of stay in zinc supplemented group as compared to placebo, but similar to our study, the difference was statistically not significant [19]. However, Brooks et al., Singh et al. and Malik et al. found significant reduction in duration of stay of patients of ALRTI after supplementation of Zinc [13][16][17].Meanwhile, Bose et al., Valentiner – Branth et al. and Yuan et al found the supplementation of zinc either had no benefit or increased the duration of stay of patients of ALRTI [14][15][18].
A similar trend is also seen while evaluating the patients in terms of oxygen requirement during treatment. While studies by Rady et al. and Brooks et al. concur with the findings of our study, studies by Bose et al. and Valentiner – Branth et al. have found no significant reduction of oxygen requirement [10][13][14][15].
When comparing the outcome of cases according to serum zinc levels, the findings of our study were in concordance with Rady et al., Brooks et al. and Basnet et al [10][13][19]. Also, a large systematic review of zinc supplementation by Mayo-Wilson et al. found that giving children zinc supplements might reduce their risk of death in general, and their risk of death due to lower respiratory tract infection [20].
Conclusion: Zinc has a significant role to play in the acquiring and progression of ALRTI in children aged 2 months to 5 years, with patients of ALRTI having significantly lower zinc levels as compared to age, sex and nutritionally matched controls. Also, the deficiency of zinc causes the patient to have a more serious form of the disease, requiring patient to be hospitalized for longer duration as well as requiring higher oxygen demands and increasing the chances of mortality by it. But, the findings of randomized trials on zinc supplementation have provided mixed results for therapeutic and prognostic value of zinc, in the light of which, there is still need of large, community based longitudinal studies. The limitations for this study were its small sample size and being a hospital based study, it did not give the actual picture of zinc deficiency in the community.
Key Message: Role of zinc in prevention of progression of acute respiratory remains doubtful in community level.
Funding: No Funding sources
Conflicts of Interest: None declared
Ethical approval: The study was approved by institutional ethics committee
References:
1) Pneumonia. UNICEF DATA. June 2018
2) Nair BT et al. Role of zinc supplementation in acute respiratory tract infections in children aged 2 to 60 months. Int J Contemp Pediatr. 2017 Sep; 4(5):1758-1762
3)Chasapis CT, Loutsidou AC, Spiliopoulou CA, Stefanidou ME.Zinc and human health: an update. Archives of Toxicology November 2011; 86(4):521-34
4)Rasheedat Mobolaji Ibraheem, AbdulWahab Babatunde Rotimi Johnson, Aishatu Ahmed Abdulkarim, Sikiru A. Biliaminu. African Health Sciences 2014; 14(1): 136-142. Serum zinc levels in hospitalized children with acute lower respiratory infections in the north-central region of Nigeria.
5)Singh T et al. Socio-economic status scales updated for 2017. Int J Res Med Sci. 2017 Jul; 5(7):3264-3267
6) Johnsen Ø, Eliasson R. Evaluation of a commercially available kit for the colorimetric determination of zinc in human seminal plasma. International Journal of Andrology. 1987 Apr 1; 10(2):435–40.
7) Elizabeth KE. Chapter on Applied Nutrition. In: Elizabeth KE. Nutrition and Child Development, 5th edition, 2015. Paras Medical Publisher; 134
8) Hussain AM, Saldanha PR, Sharma D et al. Estimation of Zinc Levels in Children with Lower Respiratory Tract Infections: A Prospective Observational Study from India. Pediatrics and Neonatal Nursing – Open Journal. 2016 Apr 18; 2(3):91–8.
9) Shakur S, Malek MA, Bano N, Islam K. Zinc Status in Well Nourished Bangladeshi Children Suffering from Acute Lower Respiratory Infection. INDIAN PEDIATRICS. 2004; 4.
10) Rady HI, Rabie WA, Rasslan HA, El Ayadi AA. Blood zinc levels in children hospitalized with pneumonia: A cross sectional study. Egyptian Journal of Chest Diseases and Tuberculosis. 2013 Oct 1; 62(4):697–700.
11)Kumar S, Awasthi S, Jain A, Srivastava R.C. et al. Blood Zinc Levels in Children Hospitalized with Severe Pneumonia: A Case Control Study. Indian Pediatrics Volume 41, 2004
12) Arıca S, Arıca V, Dag H, Kaya A, Hatipoglu S, Fenercioglu A, et al. Serum zinc levels in children of 0–24 months diagnosed with pneumonia admitted to our clinic. Int J Clin Exp Med. 2011 Sep 15; 4(3):227–33.
13) Brooks WA, Yunus M, Santosham M, Wahed M, Nahar K, Yeasmin S, et al. Zinc for severe pneumonia in very young children: double-blind placebo-controlled trial. The Lancet. 2004 May 22; 363(9422):1683–8.
14) Bose A, Coles CL, Gunavathi, John H, Moses P, Raghupathy P, et al. Efficacy of zinc in the treatment of severe pneumonia in hospitalized children <2 y old. The American Journal of Clinical Nutrition. 2006 May 1; 83(5):1089–96.
15) Valentiner-Branth P, Shrestha PS, Chandyo RK, Mathisen M, Basnet S, Bhandari N, et al. A randomized controlled trial of the effect of zinc as adjuvant therapy in children 2–35 mo of age with severe or nonsevere pneumonia in Bhaktapur, Nepal. The American Journal of Clinical Nutrition. 2010 Jun 1; 91(6):1667–74.
16) Singh AK, Sultan MA. Comparing the Effects of Zinc Supplementation as Adjunct to the Conventional Therapy and Placebo on Morbidity in Children with Pneumonia between Ages 1 Year to 5 Years. Journal of Pediatric Care 2017 May 31
17) Malik A, Taneja DK, Devasenapathy N, Rajeshwari K. Zinc Supplementation for Prevention of Acute Respiratory Infections in Infants: A Randomized Controlled Trial. Indian Pediatrics. Volume 51, October 15, 2014
18) Yuan X, Qian S-Y, Li Z, Zhang Z-Z. Effect of zinc supplementation on infants with severe pneumonia. World Journal of Pediatrics. 2016 May; 12(2):166–9.
19) Basnet S, Shrestha PS, Sharma A, Mathisen M, Prasai R, Bhandari N, et al. A Randomized Controlled Trial of Zinc as Adjuvant Therapy for Severe Pneumonia in Young Children. Pediatrics. 2012 Apr 1; 129(4):701–8.
20)Mayo-Wilson E, Junior JA, Imdad A, Dean S, Chan XHS, Chan ES, Jaswal A, Bhutta ZA. Zinc supplementation for preventing mortality,morbidity, and growth failure in children aged 6months to 12 years of age.Cochrane Database of Systematic Reviews 2014, Issue 5. Art. No.: CD009384.
Issue: April – June 2019 [Volume 8.2]