Assessment of The Impact Of Acne Vulgaris On The Quality Of Life Of Pre-Adolescents In Navi-Mumbai
Original Research
Corresponding Author: Pranjal Ahire,Assistant Professor,Department of Dermatology,MGM Medical College & Hospital,Kamothe, Navi Mumbai- 410209, Maharashtra, India,Ph: 9004648387,Email: drpranja2013@gmail.com
Received: 22thMarch, 2019; Reviewed: 11th June, 2019; Accepted :29th June ,2019.
Citation of article: Shylaja Someshwar, Pranjal Ahire, Ramagauri Pawar, Nimain Mohanty. Assessment of the impact of acne vulgaris on the quality of life of pre-adolescents in Navi-Mumbai.New Indian Journal of Pediatrics, 2019;8.2: Page —
Original Research
![]()
Abstract :
Background: Preadolescent acne can have a detrimental effect on the psychological wellbeing of school going children which can greatly impair their quality of life.
Aim of the study: The aim of this study was to assess the impact of acne vulgaris on the Quality of life of preadolescents in Navi Mumbai through school surveys.
Methods: The study was a cross sectional questionnaire based study in two higher secondary, semi-English schools in Navi Mumbai. 507 students aged between 9-14 years were included in the study. Acne vulgaris was graded using a simple grading system from Grade1-4. The participants were asked to fill in three self- reporting questionnaires: The CADI (Cardiff acne disability index), The CDLQI (Children’s life quality index) and a short demographic data.
Results: Out of the total of 507 higher secondary school going children (9-14 years) from class 5 to 9, only students who reported acne (216) were included into the data analysis. In our study, 51.38% were females and 48.61% were males, with equal sex distribution. Grade I acne was the most common type of acne (72.2%). There was no significant association between acne severity and gender (p< 0.8933). 55.5% of the pre- adolescents had particular difficulties in the areas of emotion (felt aggressive, frustrated) and 17.1% had social interference/difficulties.
In our study, the most common Children’s Dermatology Life Quality Index (CDLQI) score observed was in the range of 0-1 (no effect) in 114 (52.7%) patients and that of The Cardiff Acne Disability Index (CADI) which an acne specific questionnaire was 0-4 (low) in 190 (87.9%) patients, which implied that the majority of them had mild psychological impact as a result of acne.
Significant association was noted between CDLQI and CADI scores and grades of acne (p<0.004 and p<0.001 respectively)
Also there was significant correlation between the CADI scores and CDQLI scores (p<0.01) which means, students who scored highly on the CDLQI also tended to score highly on the CADI .
Conclusion: The assessment of impact of acne on the QoL (Quality of life) is essential, to detect those patients who are at increased risk of being negatively affected so as to treat them in a more integrated manner. Hence it is important for health professionals to incorporate QoL measurements when managing acne patients to provide a holistic approach to their management.
Key Words: Acne, preadolescent age, Quality of Life indices.
Introduction:
Acne is a chronic inflammatory disease of the pilosebaceous units resulting from the interplay of multiple factors such as androgen-induced increased sebum production , inflammation, altered keratinisation and bacterial colonisation of hair follicles by Propionibacterium acnes. It affects almost 85% of people 12–24 years of age.1 Though it is not a life threatening illness, it forms a major chunk of dermatological practice as it occurs at a crucial age when the adolescents are undergoing a lot of social, physical and psychological changes and want to have a spotless face. It is impossible to assess its psychological and social impact in a particular individual by clinical assessments alone. Epidemiological studies can be a helpful tool to identify risk factors in a community, to quantify the burden of acne and other skin diseases and contribute to health care planning.2 The development of psychometric scales to measure the impact of disease on abstract concepts and the notion of Quality of Life (QoL) has facilitated greater understanding of the impact of acne on psychological well-being and socialization.3 Thus we decided to undertake this study through school surveys to assess its impact on acne on the adolescents’ psyche through the assessment of health related quality of life (HRQoL) in patients suffering from acne. This was done using two well established questionnaires , CDLQI (Children’s life quality index), a specific and practical measure and CADI(Cardiff Acne Disability Index ).
Materials and methods :
The study was a cross sectional questionnaire based study conducted between January 2015 to September 2017 in two higher secondary, semi-English schools in Navi Mumbai after obtaining consent from the parents through a letter written to the Principals of the schools. The permission was also obtained from the Institutional ethics committee. Participation was voluntary, and students were free to refuse to be a part of the study. 507 students aged between 9-14 years were included in the study and students with any known major medical illness were excluded.
Acne vulgaris was graded using a simple grading system as follows:4
- Grade 1 ‑ comedones, occasional papules
- Grade 2 ‑ papules, comedones, few pustules
- Grade 3 ‑ predominant pustules, nodules, abscesses
- Grade 4 ‑ mainly cysts, abscesses, widespread scarring.( Figure 1)
They were asked to fill in anonymously the 3 self- reporting questionnaires: The CADI 5(Cardiff acne disability index), The CDLQI5 and a short demographic data which included questions on name, age, sex, class, presence of acne and any other skin disease.
CADI is a well validated, self reported questionnaire consisting of five questions with a Likert scale and four response categories (0-3). The five questions relate to feeling of aggression, frustration, interference with social life, avoidance of public changing facilities, and appearance of the skin all over the last month and an indication of how bad the acne is now. The final score ranges from 0 to 15. CADI scores were graded as low (0-4), medium (5-9), and high 10-15. High scores indicate a higher level of disability. CADI identifies the area of concern in patients with acne. The patient’s response to the questionnaire is significantly correlated with the clinician’s assessment of acne severity.6
CDLQI is a validated questionnaire which grades QoL by assessing the following domains:
(a) physical symptoms and feelings (questions 1 and 2), (b) daily activities (questions 3 and 4), (c) leisure (questions 5 and 6), (d) work/school (questions 7), (e) personal relationships (questions 8 and 9), and (f) treatment (question 10). Each question is scored as “very much” (score 3), “a lot” (score 2), “a little” (score 1), and “not at all” (score 0), keeping in mind the problems faced in the previous week due to the disease. Final CDLQI score is the sum of all scores (range: 0–30). High scores indicate poor QoL. Results from 0 to 1 mean no effect of the disease on the patient’s QoL, 2–5 mean small effect, 6–10 mean moderate effect, 11–20 mean great effect, and 21–30 mean a very important effect7.
Statistical analysis:
Data was entered into MS-Excel sheet and was analysed using statistical package IBM SPSS 21.0. The Data is presented using frequency, percentage and descriptive statistic such as mean, SD and SEM. Further statistical analysis was carried out using statistical tests such as Chi-square test. Microsoft word and Excel were used to generate graphs and tables.
The level of significance was set at 5%. P values less than 0.05 were considered to be statistically significant.
Results:
A total of 507 higher secondary school going children (9-14 years) from class 5 to 9 fulfilling the inclusion and exclusion criteria were taken in the study. The numbers of completed questionnaires returned were 487, a response rate of 96.0% while 20 (3.9%) questionnaires were incomplete. Overall, 44.3% (216/487) of students’ self- reported acne. Only students who reported acne (216) were included into the data analysis.
All the students with self – reported acne were screened for the severity of acne. Out of 216 children with acne, 111(51.4) were females and 105(48.6) were males. The frequency of acne was highest at 13 years of age in both males (34.3%) and females (38.7%) followed by 14 years (35.2% in males and 35.13% in females).
Acne grading:
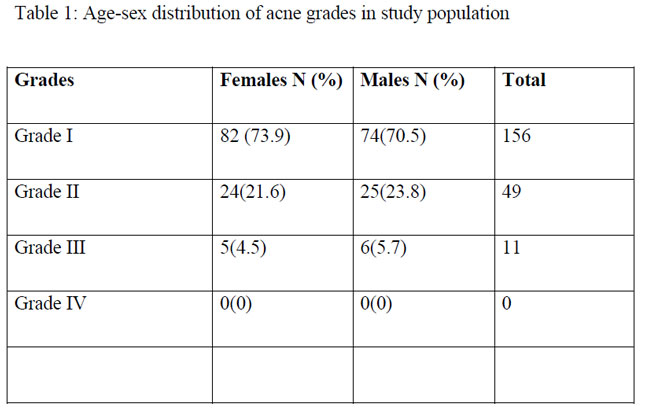
Grade I was the most common type of acne (72.2%) followed by grade II (22.8%) and grade III (5.0%). None had grade IV acne (Table 1). No significant difference in acne grades between both sexes was observed. 83 (73.8%) females and 77 (73.3%) males had grade I acne; 24 (21.6%) females and 23 (21.9%) males had grade II acne and; 5 (4.5%) females and 5 (4.7%) males had acne. None had grade IV acne.(figure 2)
Scoring of Acne Based on Children’s Dermatology Life Quality Index:
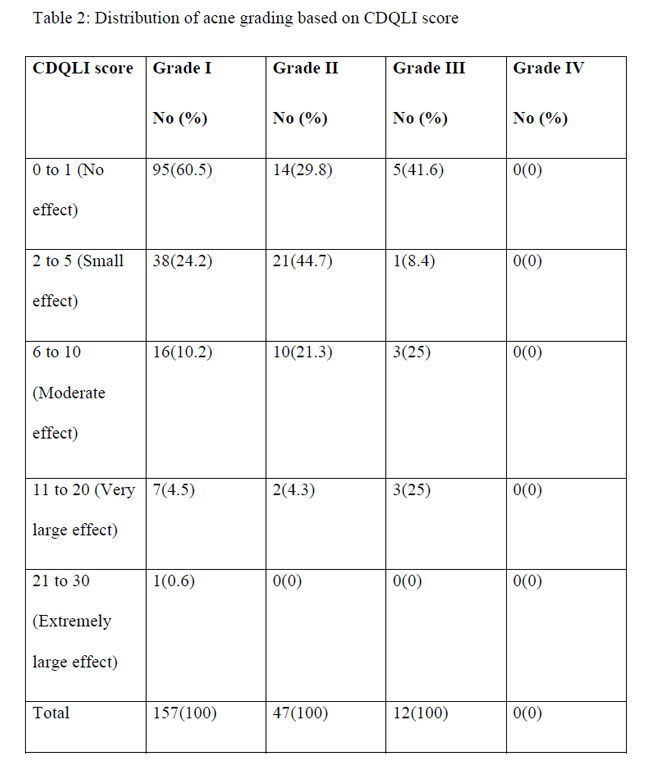
There was no significant differences in the CDQLI scores between males and females. Mean CDQLI was 1.29 which was low. The most common CDLQI score observed was in the range of 0-1 (no effect) in 114 (52.7%) patients. 29 students scored between 6 and 10 suggesting moderate HRQoL impairment and 11 scored > 10 indicating severe impairment (Table 2)
CADI:
190 (87.96%) patients scored between 0 to 4, which indicates that acne had low effect on the students as a result of acne, as it is an acne specific questionnaire. Out of these 190 students, 149 (78.4%) hade grade I acne; 35 (18.42%) had grade II acne and; 6 (3.15%) had grade III acne. (Table 3) There was no remarkable differences in the CADI scores between both the sexes.
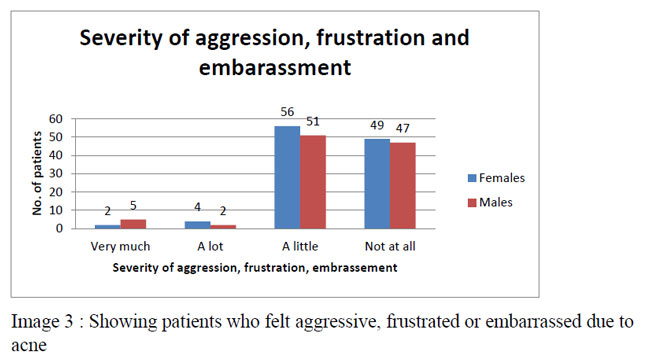
In the study population 2(1.8%) females and 5(4.8%) males showed very much; 4 females (3.6%) and 2(1.9%) males showed a lot and 49 (44.1%) females and 47 (44.8%) males showed a little aggression, frustration and embarrassment as a result of acne. (Figure 3)
On correlating the same with the grades of acne, 1 patient with grade I acne, 4 patients with grade II acne and 2 patients with grade III felt severe; 2 patients with grade I acne, 3 patients with grade II acne and 1 patient with grade III acne felt moderate and; 73 patients with grade I acne, 28 patients with grade II acne and 4 patients with grade III acne felt mild aggression, frustration and embarrassment as a result of acne. (Table 4)
The specific responses of CADI has been shown in table 5
Discussion:
Adolescence is a time of physical, emotional, and social development. Acne is a common adolescent problem, affecting more than 85% of teenagers, as well as some adults 8. With the early onset of puberty the number of cases with preadolescent or childhood acne is on the rise and the cause for significant psychological and social impact. Hence, it is important to assess the impact of acne in school going children.
The age group of acne vulgaris patients included in different studies done in this regard is variable. Most of the studies[8-12] have included an age group between 13 and 18 years and some studies[13-16] from 11 years and some[17,18] from 17 years. The present study included age group between 9 and 14 years. To the best of our knowledge, this study in pre-adolescents is been done for the first time.
In our study, total of 216 patients of Acne fulfilling the inclusion criteria were included in the statistical analysis. This study showed similar sex distribution (female: male ratio of 1.1:1) which is in contrast to other studies of different age groups,[7, 8, 19-22] where majority of the study population were females which may be because females are more conscious of their appearance than the males. In our study, highest incidence of acne was seen at 13 years of age (36.6%) followed by 14 years (35.2%). We had higher prevalence of Grade I acne (156, 72.2%), which was less than that reported by Durai PC, Nair DG[19] (age group 13 to 18 years, 95%). Amongst the severity of acne, 73.9% (82/111) females had Grade I acne and 70.5% males (74/105) had grade I acne; followed by grade II 21.6% females and 23.8% males; grade III 4.5% females and 5.7% males; none had grade IV acne. However, male students were found to have slightly more moderately severe acne compared to female students. The findings are consistent with previous studies done in other countries.[10,11] Males tend to have more severe acne compared to females because they have oilier complexion and their androgen levels are higher.[10]
In our study, mean CDQLI was 1.29 which was low. Other previous studies performed among adolescents in other countries have also reported similar findings.[11,12,] 29 students scored between 6 and 10 suggesting moderate HRQoL impairment and 11scored > 10 indicating severe impairment. The overall mean CADI score (max. 15) of 1.21 was low, but 24 students scored between 5 and 9, 3 scored >10. Relatively low scores may demonstrate the predominance of clinically mild acne in the community setting. However, these scores were low as compared to the studies in adolescents by Jankovic et al (3.75)[1], Belliappa PR et al (4.8)[8] and Durai PC, Nair DG (5.2),[19] but was in accordance with the study by Walker et al[13] (1.9). However, the fact that all the students completed questionnaires together in the same classroom, with their peers being able to read their answers, may have prevented some of them to express how they really felt.
In our study, there was no statistical significance between acne severity and gender (p<0.8933), which states that acne severity was same between males and females and both were concerned about their acne.
CADI helps to assess the QoL in students with acne. The subscales include feeling of aggression, frustration, interference with social life, avoidance of public changing facilities, and appearance of the skin. In this study, analysis of the subscales showed that 55.5% of the pre- adolescents had particular difficulties in the areas of emotion (felt aggressive, frustrated), and 17.1% had social interference/difficulties. 7% avoided public changing facilities all or most of the time. 19.4% avoided swimming and other sports because of their acne. Also 7.2% females and 4.8% males were depressed and felt miserable as a result of acne. In our study, acne was reported as worst problem in 5.4% of females and in 2.9% of males; a major problem in 2.7% females and 4.8% males and a minor problem in 46.8% females and 35.2% of males in the affected study population. This indicates that females had more psychological than males.
Belliappa PR and Umashankar N[8] reported that 60.7% of the adolescents had particular difficulties in the areas of emotion (felt aggressive, frustrated), 43.6% had social interference/difficulties and 60.7% of the adolescents reported that they felt aggressive, frustrated, or embarrassed as a result of having acne.
Hanisah et al.[10] reported difficulties in the areas of emotion (felt aggressive, frustrated) in 71% of adolescents and social interference/difficulties in 58.7% of adolescents.
A study among teenage Scottish school[11] children reported that 50% of students were emotionally affected, 20% of pupils were affected in their personal and social lives, and 10% avoided swimming and other sports because of their acne. In a study by Jankovic et al[9] 15% of pupils felt very depressed and miserable due to their acne.
In our study, 190 (87.9%) students scored 0–4, 24 (11.1%) scored 5-9 and 3 (1.38%) students scored 10-15 in CADI. This implied that, over all, the students were mildly affected psychologically. This could be due to the higher prevalence of mild acne among pre -adolescent which was in accordance with other studies done in adolescents.[8,10]
The most common CDLQI score observed was in the range of 0-1 (no effect) in 114(52.7%) patients and that of CADI was 0-4 (low) in 190 (87.9%) patients, which implied that the majority of them had mild psychological impact as a result of acne. Statistically significant association was noted between CDLQI and CADI scores and grade of acne (p < 0.004 for CDLQI & p <0.001 for CADI respectively). The impact on quality of life increased with the facial acne severity.
There was no statistically significant association noted between CDLQI and CADI scores and gender (p= 0.5 for CDLQI & p= 0.5 for CADI respectively). This is an important finding, as there may be a general perception that facial acne will have less impact on boys and also stresses the fact that boys also experience psychological morbidity and were concerned about their acne.
Also there was significant correlation between the CADI scores and CDQLI scores (p<0.01) which means, students who scored highly on the CDLQI also tended to score highly on the CADI.
Conclusion:
In our study, facial acne was found to be common among pre- adolescent group and can cause major impact on their quality of life. Most of the pre-adolescents reported that they felt aggressive, frustrated or embarrassed as a result of having acne. Thus assessment of impact of acne on the QoL is essential, to detect those patients who are at increased risk of being negatively affected so as to treat them in a more integrated manner. It is essential for health professionals to incorporate QoL measurements when managing acne patients to provide adequate and appropriate care. In addition, both CADI and CDQLI scales were easy to administer and an easy tool to assess the psychosocial impact of acne.
Key Message: It is essential for health professionals to incorporate QoL measurements when managing acne patients to provide adequate and appropriate care.
Conflict of interest: None
Funding: None
References:
1. Krowchuck DP. Managing Acne in Adolescent. Pediatr Clin North Am 2000;47(4):841–857.
2. Tasoula E, Gregoriou S, Chalikias J, Lazarou D, Danopoulou I, Katsambas A, et al. The impact of acne vulgaris on quality of life and psychic health in young adolescents in Greece. Results of a population survey. An Bras Dermatol 2012;87:862-9.
3. Tan JK. Psychosocial impact of acne vulgaris: evaluating the evidence. Skin Therapy Lett 2004; 9: 1-9.
4. Adityan B, Kumari R, Thappa DM. Scoring systems in acne vulgaris. Indian J Dermatol Venereol Leprol 2009;75:323-6.
5. Motley RJ, Finlay AY. Practical use of a disability index in the routine management of acne. Clinical and Experimental Dermatology 1992; 17: 1-3. (Department of Dermatology. CADI Information and Instructions- Department of Dermatology-Cardiff University. http://sites.cardiff.ac.uk/drmatology/quality-of-life/cardiff-acne-disability-index-cadi/cadi-information-and-instructions/)
6. Hanisah A, Omar K, Shah SA. Prevalence of acne and its impact on the quality of life in school‑aged adolescents in Malaysia. J Prim Health Care 2009;1:20-5.
7. Tasoula E, Gregoriou S, Chalikias J, Lazarou D, Danopoulou I, Katsambas A, et al. The impact of acne vulgaris on quality of life and psychic health in young adolescents in Greece. Results of a population survey. An Bras Dermatol 2012;87:862-9.
8. Belliappa Pemmanda Raju, Umashankar Nagaraju. Quality of life among adolescents with acne in a tertiary referral centres in Bangalore, South India. Indian journal of Paediatric Dermatology 2017; 18:94-99
9. Jankovic S, Vukicevic J, Djordjevic S, Jankovic J, Marinkovic J. Quality of life among school children with acne: Results of a cross sectional study. Indian J Dermatol Venerol Leprol 2012;78:454-8.
10. Hanisah A, Omar K, Shah SA. Prevalence of acne and its impact on the quality of life in school-aged adolescents in Malaysia. J Prim Health Care 2009;1:20-5.
11. 28. Walker N, Lewis-Jones MS. Quality of life and acne in Scottish adolescent schoolchildren: Use of the Children’s Dermatology Life Quality Index (CDLQI) and the Cardiff Acne Disability Index (CADI). J Eur Acad Dermatol Venereol 2006;20:45-50.
12. Pawin H, Chivot M, Beylot C, Faure M, Poli F, Revuz J, et al. Living with acne. A study of adolescents’ personal experiences. Dermatology 2007;215:308-14
13. Uslu G, Sendur N, Uslu M, Savk E, Karaman G, Eskin M. Acne: Prevalence, perceptions and effects on psychological health among adolescents in Aydin, Turkey. J Eur Acad Dermatol Venereol 2008;22:462-9
14. Jones-Caballero M, Chren MM, Soler B, Pedrosa E, Peñas PF. Quality of life in mild to moderate acne: Relationship to clinical severity and factors influencing change with treatment. J Eur Acad Dermatol Venereol 2007;21:219-26
15. Rapp SR, Feldman SR, Graham G, Fleischer AB, Brenes G, Dailey M. The Acne Quality of Life Index (Acne-QOLI): Development and validation of a brief instrument. Am J Clin Dermatol 2006;7:185-92.
16. Ismail KH, Mohammed-Ali KB. Quality of life in patients with acne in Erbil city. Health Qual Life Outcomes 2012;10:60.
17. Lasek RJ, Chren MM. Acne vulgaris and the quality of life of adult dermatology patients. Arch Dermatol 1998;134:454-8.
18. Balkrishnan R, McMichael AJ, Hu JY, Camacho FT, Shew KR, BoulocA, etal. Correlates of health-related quality of life in women with severe facial blemishes. Int J Dermatol 2006;45:111-5.
19. Durai PC, Nair DG. Acne vulgaris and quality of life among young adults in South India. Indian Journal of Dermatology 2015;60:33-40
20. Aghaei S, Mazharinia N, Jafari P, Abbasfard Z. The Persian version of the Cardiff Acne Disability Index. Reliability and validity study. Saudi Med J 2006;27:80-2.
21. Rapp DA, Brenes GA, Feldman SR, Fleischer AB Jr, Graham GF, Dailey M, et al. Anger and acne: Implications for quality of life, patient satisfaction and clinical care. Br J Dermatol 2004;151:183-9.
22. Tasoula E, Gregoriou S, Chalikias J, Lazarou D, Danopoulou I, Katsambas A, et al. The impact of acne vulgaris on quality of life and psychic health in young adolescents in Greece. Results of a population survey. An Bras Dermatol 2012;87:862-9.
Images:

- A: Grade I(Mild)
- B: Grade II(Moderate)
- C: Grade III(Severe)
- D: Grade IV (Cystic)

Tables



Issue: April – June 2019 [Volume 8.2]