Recurrent Respiratory Tract Infection – Expecting The Unexpected! Jarcho Levine syndrome
Case report
Corresponding Author: Dr. Vikas Gupta ,Assistant Professor,MGM Medical Collge Kamothe ,Navi Mumbai-410209.Email- guptavkas01@gmail.com
Received: 7, April, 2019; Reviewed: 30, April, 2019; Accepted: 16, May, 2019.
Citation of article: Neha Pandey, Vikas Gupta, R Keshwani, H Uchil, S Zope, Radha Ghildiyal. Recurrent Respiratory Tract Infection – Expecting The Unexpected! Jarcho Levine syndrome New Indian Journal of Pediatrics, 2019; 8.3.
Case report
![]()
Abstract: Jarcho Levine syndrome is a rare genetic defect characterised by multiple malformation of ribs and vertebrae. The syndrome has been described in two major subtypes: Spondylothoracic dysostosis and spondylocostal dysostosis. Infants affected with this syndrome have higher rate of recurrent respiratory infections.
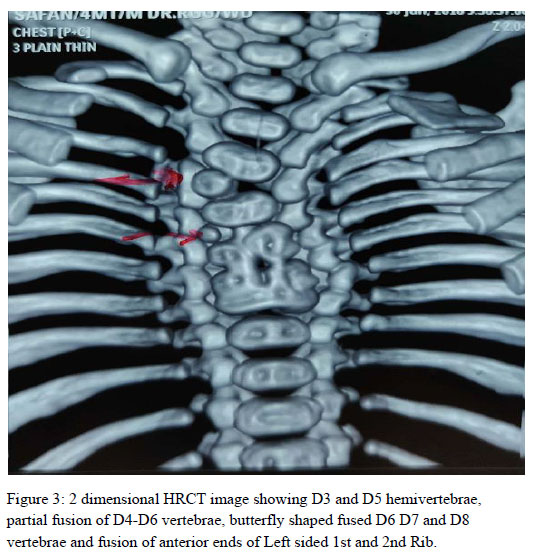
We present here a case of 4 month old boy, born of 3rd degree consanguineous marriage presented to us with history of cough, cold and fast breathing. He had history of recurrent lower respiratory tract infections requiring mechanical ventilation and extensive intravenous antibiotics. Skiagram showed Scoliosis, crab like chest deformity with fusion of anterior 1st and 2nd ribs on the left side. A 2 dimensional high resolution chest tomography showed areas of consolidation in posterior segment of right upper lobe and apicoposterior segment of left upper lobe consistent with the clinical findings. There were D3 and D5 hemi vertebrae with D6, D7, D8 butterfly vertebrae and partial fusion of D4-D6 to D7-D8 vertebrae and fusion of posterior elements of D3-D4 vertebrae on left side.
Keywords: Jarcho Levine syndrome, crab like chest deformity, butterfly vertebrae, recurrent lower respiratory tract infections
Introduction: Jarcho Levine syndrome is a rare genetic defect characterised by multiple malformation of ribs and vertebrae. This syndrome was first described in 1938 by Jarcho and Levin. The syndrome has been described in Two major subtypes : Spondylothoracic dysostosis and spondylocostal dysostosis. infants affected with this syndrome have higher rate of recurrent respiratory infections.(1)
Case Scenario: A 4 month old boy, born of 3rd degree consanguineous marriage presented to us with history of cough, cold and fast breathing. He was a preterm, born at 31 weeks of gestation with a birth weight of 1.2 kg and had a history of NICU stay for respiratory distress and preterm care and discharged at corrected gestational age of 39 weeks with weight of 2.47kg, immunised completely for age and had also received pneumococcal conjugate vaccine. He had history of recurrent lower respiratory tract infections requiring mechanical ventilation and extensive intravenous antibiotics.
He weighed 4.6kg and length of 55cm with a US/LS ratio of 0.96. Child had plagiocephaly with short neck, protuberant abdomen, sacral dimples and mongoloid spots.

At the time of presentation, he was tachycardiac and tachypneic with respiratory distress in the form of subcostal and intercostal retractions. Air entry was reduced bilaterally and coarse crepitations were present.
He had respiratory alkalosis with hypoxemia and microcytic hypochromis anemia with haemoglobin of 9.9 g/dl. Peripheral smear showed microcytes, macrocytes, anisocytes. His other blood counts and kidney and liver functions were normal. Skiagram showed Scoliosis, crab like chest deformity with fusion of anterior 1st and 2nd ribs on the left side.

A 2 dimensional high resolution chest tomography showed areas of consolidation in posterior segment of right upper lobe and apicoposterior segment of left upper lobe consistent with the clinical findings. There were D3 and D5 hemi vertebrae with D6, D7, D8 butterfly vertebrae and partial fusion of D4-D6 to D7-D8 vertebrae and fusion of posterior elements of D3-D4 vertebrae on left side. A 2D echo revealed tiny closing atrial septal defect with No pulmonary artery hypertension. Abdominal ultrasonography showed no significant abnormality and normal renal anatomy.


The child is currently following up in Outpatient department and has not developed signs of lung failure as of now and has been advised conservative management by orthopedics department.
Discussion: Jarcho-Levin syndrome is a rare genetic disorder with autosomal dominant (AD) or autosomal recessive (AR) inheritance. The gene disorder is associated with autosomal dominant (AD) or autosomal recessive (AR) inheritance. The gene affected in this syndrome is delta-like protein 3 (DDL3) on chromosome 19 at 19q13,5 and mesoderm posterior protein 2 (MESP2) gene located on chromosome 15 at 15q26.1.6(1) Spondylocostal dysplasia is caused by a change (mutation) in one of at least five different genes, specifically the DLL3, MESP2, LFNG, HES7, and TBX6 genes(2)
Type 1 (spondylothoracic dysostosis) is the more severe form associated with severe spine involvement and respiratory failure and it is inherited as Autosomal recessive pattern. Type ll (spodylocostal dysostosis) is a milder form, has AD inheritance and is difficult to diagnose in utero. They have near normal longevity. There is equal sex preponderance in both types. (1)
Diagnosis is usually made on radio-clinical examination. Confirmation can be made with Gene Sequencing however, the disease being rare genetic study is available in specialised laboratories.
Distinctive radiographic findings of Spondylothoracic dysostosis include: abnormal segmentation of all vertebral segments with ‘‘H-shaped vertebrae’’ and shortening of the spine, fusion of various vertebrae, especially in the dorsal area. The anteroposterior radiograph shows fan-shaped ribs from the costovertebral base, giving it a ‘‘crab-like’’ appearance. Due to extensive costal fusion, the intercostal muscles are not able to expand the thorax leading to decreased lung capacity and chronic lung failure.(3) Usually above features lead to neonatal mortality, however our case presented to us with a recurrent respiratory tract infection and skiagram was suggestive of crab like chest and Scoliosis.
Spondylocostal dysplasia can vary greatly from one person to another, affected individuals have abnormalities in the development of the spine and ribs. Scoliosis occurs in one third of the patients. Rib anomalies include absence, posterior fusion and irregular size and shape.(4) The bones of the spine (vertebrae) may be fused together or partially be fused. They are underdeveloped and wedge-shaped (hemivertebrae). Multiple vertebrae are always affected, The ribs may be fused together, misaligned, split or forked (bifid), and sometimes some of the ribs are missing. (2)
Scoliosis is usually mild to severe. Scoliosis should be carefully followed with spine x-rays. Affected infants and children cannot expand their chests sufficiently with causes reduced lung capacity, due to multiple thoracic cage and rib defects, which means the lungs holds less air than they normally would. Therefore, they have predisposed to difficulty in breathing and have repeated respiratory infections, which are known as thoracic insufficiency syndrome. Pulmonary hypertension is a chronic and, if not treated, life-threatening complication found in such cases. Reduced lung capacity also increases the risk of heart failure which is another serious effect. (2)
Most cases with SCD have a good prognosis, due to in part to the asymmetry of the thoracic anomalies resulting in a less restrictive chest. In patients with STD mortality is of 45%. (5)
Most of the cases are born out of consanginous marriage and are diagnosed in newborn life; our case was diagnosed on the basis of radio- clinical examination at the age of 4 months.
Pediatric surgery and orthopedic evalaution are necessary during patient follow-up subsequent for the surgical planning of scoliosis, costal fusions, though malformation treatment is conservative in most cases, with periodical radiographic controls, physiotherapy and infection control. (3)
Child was advised regular follow up (3 monthly) with serial X- rays and a conservative line of management was observed. The child is thriving well and does a regular follow up in outpatient care services.
Conclusion: Jarco Levine syndrome is rare disorder that is characterised by multiple Vertebral and rib cage anomalies leading to Decreased thoracic capacity which can lead to recurrent lower respiratory tract infections. Since most severe respiratory problems in patients with STD are related to mechanical restriction, early and aggressive management of respiratory infections is very important to improve their prognosis. A high index of suspicion should be kept in early infants presenting with bony defects or Radiographic features due to complications associated with this syndrome. Children with STD have incidences of earlier and high mortality.
Declaration:
Contribution of authors: All authors participated in the analysis of the presented case report.
Conflict of Interest: None
Ethical Approval: The study approved by the Institutional Ethics Committee
Funding: Self
References:
1. Bindu CM, Krishnappa J, Hegde P BM. Jarcho-Levin syndrome (spondylocostal dysostosis) associated with Sprengel deformity [Internet]. 2017 [cited 2018 Jul 31]. Available from: http://dx.doi.org/10.15380/2277-5706.JCSR.16.03.005.
2. Scdo SCD. Synonyms of Spondylocostal Dysplasia Signs & Symptoms. :1–9.
3. Medina-De La Cruz AY, Rodríguez-Balderrama I, Burciaga-Flores CH, Martínez-De Villarreal LE, Ibarra-Ramírez M, De La O-Cavazos ME. Spondylothoracic dysostosis, Jarcho Levin syndrome. Case report. Med Univ [Internet]. 2016 [cited 2018 Jul 31];18(70):16–9. Available from: www.elsevier.es/rmuanl
4. Vázquez-López ME, López-Conde MI, Somoza-Rubio C, Pérez-Pacín R, Morales-Redondo R, González-Gay MA. Anomalies of vertebrae and ribs: Jarcho Levin syndrome. Description of a case and literature review. Jt Bone Spine. 2005;72(3):275–7.
5. Cornier AS, Ramírez N, Arroyo S, Acevedo J, García L, Carlo S, et al. Phenotype characterization and natural history of spondylothoracic dysplasia syndrome: A series of 27 new cases. Am J Med Genet. 2004;128 A(2):120–6.
Issue: July-September 2019 [Volume 8.3]