Corresponding author: Dr.Alka Singh, e mail id: dralka24@yahoo.in, mob no:9835217017
RECEIVED: 15 TH October, 2018. REVIEWED: 26 th December v2018. ACCEPTED: 5 th January, 2019
Abstract:Background: Jaundice is one of the most common conditions requiring medical attention in newborn babies. Exchange transfusion is standard method of therapy for immediate treatment of severe hyperbilirubinemia and prevention of kernicterus. As bilirubin is removed from plasma, extra vascular bilirubin equilibrates and binds to albumin in exchanged blood. Within half hour of exchange transfusion bilirubin level returns to 60% of pre exchange level. Guidelines for the implementation of phototherapy and exchange transfusion rely on evidence-based estimates of when the benefit of these interventions exceeded their risks and costs.
Material and methods: The following study is a prospective study carried out in Hospital for Children and Upgraded Department of Paediatrics, PMCH, Patna. Neonates who underwent exchange transfusion for neonatal hyperbilirubinemia from August 2011 to September 2012 in NICU were included in study.
Result: In this study most common cause of hyperbilirubinemia requiring exchange transfusion was ABO incompatibility i.e 42.86%, (n=15). Rh incompatibility constituted 22.85% of cases (n=8). In remaining 34.29% cases (n=12) no specific cause could be found. Immediate complications were seen in 7 out of 35 cases (20%). all cases were followed till age of 12 months, at 6 months follow up, out of 34 cases 4(11.76%) showed gross motor and fine motor delay while language and social personal delay was seen in 2(5.88%) and 3(8.82%) respectively. At 12 months follow up out of remaining 32 cases (3 were lost to follow up) 4 cases (12.5%) showed delay in developmental milestones.
Conclusion: Two most common cause for hyperbilirubinemia needing exchange transfusion are ABO incompatibility (42.86%) and Rh incompatibility (22.85%). In about 34.29% of cases exact cause could not be found out. Pre exchange bilirubin values strongly correlated with persistent BERA changes (p value<0.005).
KEY WORDS: Exchange transfusion,Neonatal hyperbilirubinemia,Kern icterus ,Rh incompatability.
INTRODUCTION: Jaundice is one of the most common conditions requiring medical attention in newborn babies. Approximately 60% of term and 80% of preterm babies develop jaundice in the first week of life, and about 10% of breastfed babies are still jaundiced at 1 month of age.
Kaplan and associates7 demonstrated that an imbalance between bilirubin production and conjugation is fundamental in the pathogenesis of neonatal bilirubinemia.
Bilirubin inhibits mitochondrial enzymes, interferes with DNA and protein synthesis6, and alters cerebral glucose metabolism4. Unconjugated bilirubin initiates a mitochondrial pathway of apoptosis in developing brain neurons8 and it inhibits the function of N methyl-aspartate-receptor ion channels5.
The region most commonly affected are the basal ganglia, particularly the subthalamic nucleus and the globus pallidus, the hippocampus, the geniculate bodies, various brainstem nuclei, including the inferior colliculus, oculomotor, vestibular, cochlear, and inferior olivary nuclei, and the cerebellum especially the dentate nucleus and the vermis2.
Exchange transfusion is standard method of therapy for immediate treatment of severe hyperbilirubinemia and prevention of kernicterus. Exchange transfusion removes partially hemolysed and antibody coated RBCs as well as unattached antibodies and replaces them with donor RBCs lacking sensitising antigen. As bilirubin is removed from plasma, extra vascular bilirubin equilibrates and binds to albumin in exchanged blood. Within half hour of exchange transfusion bilirubin level returns to 60% of pre exchange level.
Exchange transfusion is generally initiated1
1) When phototherapy fails to prevent rise in bilirubin to toxic levels
2) To correct anaemia and improve heart failure in hydropic infants with haemolytic disease.
3) To stop haemolysis and bilirubin production by removing antibody and sensitized RBCs.
4) In haemolytic disease, immediate exchange is needed when:-
- Cord bilirubin level >4.5mg/dl and cord haemoglobin level <11g/dl.
- Bilirubin level is rising >1mg/dl despite phototherapy
- Haemoglobin level is between 11g/dl and 13g/dl, and bilirubin level is rising >0.5mg/dl despite phototherapy.
- Bilirubin level is 20mg/dl or appears to reach 20 mg/dl at the rate it is rising
- There is progression of anaemia in face of adequate control of bilirubin by other methods.
The bilirubin level at which intervention is necessary is still a contentious issue. Various study groups had proposed guidelines regarding initiation of exchange transfusion. Guidelines for the implementation of phototherapy and exchange transfusion rely on evidence-based estimates of when the benefit of these interventions exceeded their risks and costs. Ideally, these estimates should come from randomized trials or high quality, systematic observational studies but such studies are rare. Thus, treatment guidelines must rely on relatively uncertain estimates of risks and benefits and the recognition that using a single TSB level to predict long-term behavioural and developmental outcomes is not reliable and will lead to conflicting results.
Design: Prospective cohort study
Setting: Carried out in Hospital for Children and Upgraded Department of Paediatrics, PMCH, Patna.
Participants: 35 newborns with exchange transfusion were followed for 12 months
MATERIALS AND METHODS: Neonates who underwent exchange transfusion for neonatal hyperbilirubinemia from August 2011 to September 2012 in NICU were included in study. Medical records of patients were reviewed and data was recorded through proper history taking, clinical methods, laboratory investigations and one year follow up. All neonates with bilirubin level compatible with levels for which exchange transfusion is indicated according to AAP nomogram were included in study. Neonates undergoing exchange transfusion due to causes other than hyperbilirubinemia were not included in study, like exchange in cases of:-
a) neonatal polycythemia
b) severe anaemia
c) neonatal sepsis
In this study, isovolaemic double volume fresh whole blood (within 7 days) was used. Exchange was done with neonate under radiant warmer and cardiac and BP monitoring in place. Umbilical vein catheterisation was done under aseptic conditions. Exchange was done with push pull technique. Removal and infusion of blood was done according to standard published guidelines with intermittent infusion of calcium. CBC, serum bilirubin levels, electrolytes, glucose were measured after exchange.
Follow up: – All infants who were included in study were followed at regular interval upto 12 months of age. BERA was done at 3 months of age, follow up and assessment during later period ( 6 months and 12 months) was done in terms of attainment of neurodevelopmental milestone under following headings:-
- Gross motor
- Fine motor
- Social personal
- Language
OBSERVATION AND RESULTS: In this study amongst 35 cases 18 (51.4%) were male and 17 (48.6%) were female. Majority (80%) of babies in this study were term (n=28), preterm (n=7) constituted only 20% of total cases. In this study most common cause of hyperbilirubinemia requiring exchange transfusion was ABO incompatibility i.e 42.86%, (n=15). Rh incompatibility constituted 22.85% of cases (n=8). In remaining 34.29% cases (n=12) no specific cause could be found. Out of 35 cases most of babies had pre exchange bilirubin level between 20.1-25.0 mg/dl (n=18; 51.43%).remaining 17 were clustered in 15.0-20.0 mg/dl (n=5; 14.29%), 25.1-30.0 mg/dl (n=6; 17.14%) and 30.1-35.0 mg/dl (n=6; 17.14%) respectively. Mean pre exchange bilirubin value was 24.53 ± 4.34 mg/dl as compared to post exchange value which was 13.68 ± 3.44 mg/dl. None of the cases underwent second exchange transfusion in this study.
OUTCOME ON FOLLOW UP: In this study follow up of neonates who underwent exchange transfusion was done for 12 months. At 3 months BERA was done to look for any residual effect of hyperbilirubinemia. Out of 35 cases 4 cases were lost to follow up, 1 at 6 months and rest 3 at 12 months. At 3 month follow up 4 cases (11.43%) showed abnormal BERA records and on further follow up all of these cases showed abnormal development.
{kind=link}
On analysis of data it was found that residual defect at 3 month of life suggested by abnormal BERA was in correlation with initial bilirubin level ( p value< 0.005)
Out of 4 cases with abnormal BERA readings 1 had absent waveform, 1 had prolonged latencies III and other 2 showed prolonged latencies V.
{kind=link}
{kind=link}
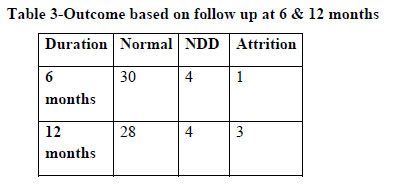
In this study all cases were evaluated at 6 and 12 months for residual defects attributed to hyperbilirubinemia. Out of total 35 cases 3 were lost to follow up (1 at 6 months and remaining 2 at 12 months). Out of remaining cases only 4 cases (11.43%) showed neurodevelopmental delay in terms of attainment of milestones of development
{kind=link}
In this study all cases were followed till age of 12 months, at 6 months follow up, out of 34 cases 4(11.76%) showed gross motor and fine motor delay while language and social personal delay was seen in 2(5.88%) and 3(8.82%) respectively.
At 12 months follow up out of remaining 32 cases (3 were lost to follow up) 4 cases (12.5%) showed delay in developmental milestones.
Discussion : In present study sample size was of 35 neonates with hyperbilirubinemia. This was comparable to sample size of Salas AA14 et al (n=56), Spada A4 et al (n=57), and Patra K8 et al (n=55).
In this study most common cause of hyperbilirubinemia requiring exchange transfusion was ABO incompatibility i.e 42.86%, (n=15). Rh incompatibility constituted 22.85% of cases (n=8). In remaining 34.29% cases (n=12) no specific cause could be found. It is mainly due to lack of investigations in our resource limited setting. This was comparable to that of studies carried out by Hosseinpour Sakha12 et al where also most common cause was ABO incompatibility (49.3%), Badiee Z13 in a similar work also concluded that most common cause of hyperbilirubinemia requiring exchange transfusion was ABO incompatibility, though it constituted 22.1% of cases. Dikshit SK3 et al also had comparable results regarding cause of exchange transfusion i.e ABO incompatibility being most common followed by Rh incompatibility.
In this study mean pre exchange bilirubin value was 24.53 ± 4.34 mg/dl as compared to post exchange value which was 13.68 ±3.44 mg/dl. None of the cases underwent second exchange transfusion in this study. 51.43% of cases had bilirubin level between 20.1-25.0 mg/dl (n=18).Similar study by Hosseinpour Sakha S12 et al showed mean pre exchange bilirubin value of 29.59 ± 6.88 mg/dl. Salas AA14 et al found mean pre exchange bilirubin value of 31.1 mg/d, this explains higher incidence of bilirubin encephalopathy in his study.
In this study all cases were followed for 12 months to study adverse effects associated with hyperbilirubinemia and exchange transfusion. BERA was done at 3 month of age. Remaining follow up was done on clinical basis due to resource limitations. Out of 35 cases 4 were lost to follow up, 1 at 6 month and rest 3 at 12 month. At 3 month follow up 4 cases (11.43%) showed abnormal BERA records and on further follow up all of these cases showed abnormal development. It is comparable to study of Agrawal et al in which 10% of cases ( n=30) had persistent BERA changes on follow up. Sharma et al10 found persistent abnormal BERA records in 16.7% of cases (n=30), where as Bhandari11 et al, Deorari9 et al, Gupta et al found no cases with abnormal BERA record on follow up indicating transient nature of bilirubin encephalopathy. In this study there was significant correlation between serum bilirubin value and persistent BERA changes (chi2=12.053; p value < 0.005) indicating that higher the bilirubin value greater is the risk of damage to auditory pathway. Study of Bhandari11et al found no correlation between serum bilirubin value and persistent BERA changes. Whereas studies of Sharma10et al, Deorari9et al, Gupta et al also showed correlation between bilirubin level >25 mg/dl and BERA changes.
Summary and conclusion : Two most common causes for hyperbilirubinemia needing exchange transfusion are ABO incompatibility (42.86%) and Rh incompatibility (22.85%). In about 34.29% of cases exact cause could not be found out. It can partly be attributed to resource limited settings in our scenario. Mean day of commencement of exchange transfusion in this study was 4.9. This delay reflects lack of early recognition of problem and scope of improvement in peripheral hospitals regarding early diagnosis of problem. Most of neonates who underwent exchange transfusion had potentially life threatening level of serum bilirubin before exchange, but on follow up only 4 of them showed persistent abnormalities in BERA, rest were normal. This strengthens the fact that exchange transfusion is very effective in rapidly reducing serum bilirubin value and in preventing kernicterus. Pre exchange bilirubin values strongly correlated with persistent BERA changes (p value<0.005), this shows that early intervention and regular monitoring are key in preventing kernicterus and permanent damage due to bilirubin encephalopathy.
DECLARATIONS:
Contributors: – Kumar Arpit – Collection of data and Analysis of the collected data, Preparation of manuscript Alka Singh -Concept, Guidance,Literature review S. R. Choudhary – Study design and Methodology, Revision of the manuscript
Competing and conflict of interests: None
Funding- None
REFERENCES:
1. GERRARD J. Kernicterus. Brain. 1952 Dec;75(4):526-70. PubMed PMID: 13009006.
2. Ahdab-Barmada M, Moossy J. The neuropathology of kernicterus in the premature neonate: diagnostic problems. J Neuropathol Exp Neurol. 1984 Jan;43(1):45-56. PubMed PMID: 6693927.
3. Dikshit SK, Gupta PK. Exchange transfusion in neonatal hyperbilirubinemia. Indian Pediatr. 1989 Nov;26(11):1139-45. PubMed PMID: 2630476
4. Spada A, Ambrosiani S. [Exsanguinotransfusion at the Holy Cross Hospital, Cuneo]. Arch Sci Med (Torino). 1969 Mar;126(3):123-8. PubMed PMID: 17342895.
5. Chuniaud L, Dessante M, Chantoux F, Blondeau JP, Francon J, Trivin F. Cytotoxicity of bilirubin for human fibroblasts and rat astrocytes in culture Effect of the ratio of bilirubin to serum albumin. Clin Chim Acta. 1996 Dec 30;256(2):103-14. PubMed PMID: 9027422.
6. Rodrigues CM, Solá S, Brites D. Bilirubin induces apoptosis via the mitochondrial pathway in developing rat brain neurons. Hepatology. 2002 May;35(5):1186-95. PubMed PMID: 11981769.
7. Kaplan M, Muraca M, Hammerman C, Rubaltelli FF, Vilei MT, Vreman HJ, Stevenson DK. Imbalance between production and conjugation of bilirubin: a fundamental concept in the mechanism of neonatal jaundice. Pediatrics. 2002 Oct;110(4):e47. PubMed PMID: 12359820.
8. Patra K, Storfer-Isser A, Siner B, Moore J, Hack M. Adverse events associated with neonatal exchange transfusion in the 1990s. J Pediatr. 2004 May;144(5):626-31. PubMed PMID: 15126997. 9. Deorari AK, Singh M, Ahuja GK, Bisht MS, Verma A, Paul VK, Tandon DA. One year outcome of babies with severe neonatal hyperbilirubinemia and reversible abnormality in brainstem auditory evoked responses. Indian Pediatr. 1994 Aug;31(8):915-21. PubMed PMID: 7883343. 10. Sharma P, Chhangani NP, Meena KR, Jora R, Sharma N, Gupta BD. Brainstem evoked response audiometry (BAER) in neonates with hyperbilirubinemia. Indian J Pediatr. 2006 May;73(5):413-6. PubMed PMID: 16741327 11. Bhandari V, Narang A, Mann SB, Raghunathan M, Bhakoo ON. Brain stem electric response audiometry in neonates with hyperbilirubinemia. Indian J Pediatr. 1993 May-Jun;60(3):409-13. PubMed PMID: 8253490.
12. Hosseinpour Sakha S, Gharehbaghi MM. Exchange transfusion in severe hyperbilirubinemia: an experience in northwest Iran. Turk J Pediatr. 2010 Jul-Aug;52(4):367-71. PubMed PMID: 21043381.
13. Badiee Z. Exchange transfusion in neonatal hyperbilirubinaemia: experience in Isfahan, Iran. Singapore Med J. 2007 May;48(5):421-3. PubMed PMID: 17453099.
14. Salas AA, Mazzi E. Exchange transfusion in infants with extreme hyperbilirubinemia: an experience from a developing country. Acta Paediatr. 2008 Jun;97(6):754-8. PubMed PMID: 18422806.
Issue: January-March 2019 [Volume 8.1]