Place of study– PICU, JIPMER Pondicherry
Address for correspondence – Dr. Sham b. Lohiya Dept. of pediatrics, 3rd floor A.V.B.R.H. Sawangi.Email- sham.lohiya19@gmail.com Mob number-8098842537
RECEIVED: 13 RD December, 2018; REVIEWED: 30 TH December, 2018; ACCEPTED: 5THJanuary, 2019
ABSTRACT: Objective of study was to assess the hand hygiene compliance in health care personnel before and after hand hygiene education and effect of change in hand hygiene compliance on rate of hospital acquired infections.
It is an observational analytical study.
Study was carried out on medical and paramedical staff working or visiting to PICU over a period of 4 months from March 2015 to June 2015.
Surveillance was done by CCTV camera recordings. Two weekly classes on hand hygiene and its importance in PICU were taken by the principal investigator
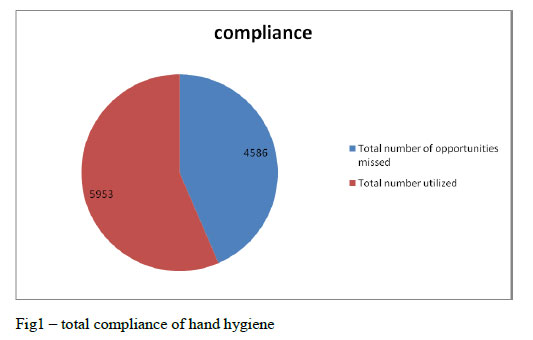
Total opportunities for HH observed during video surveillance were 10519, out of which 5953 opportunities were used with total compliance of 56%. Hand hygiene compliance in the same period i.e. Mar 2014 to June 2014 was 33%.This is a pre intervention data Hence we can see that compliance improved from 33% to 56% which is significant with p- value < 0.01.Ventilator associated pneumonia (VAP) rate between march 2014 – June 2014 was 22.3/1000 ventilation days. Central line associated blood stream infection ( CLABSI) during the same period was 10.06/ 1000 catheter days( unpublished data). In intervention phase i.e. march 2015 to June 2015, there was significant fall in VAP rate which was 13.42/ 1000 ventilator days, and CLABSI rate which was 2.78/1000 catheter days. There was significant fall in a rate of HAI.
It can be concluded that rate of hand hygiene compliance can be increased significantly by reinforcing its importance repeatedly to medical staff working in I.C.U.s. Only increase in hand hygiene compliance can decrease the number of rate of hospital acquired infections.
INTRODUCTION: Infections by multidrug-resistant organisms (MDROs) are increasing worldwide [1].Worldwide, the most common bacteria causing health-care associated infections (HAIs) are:
MRSA Methicillin resistant Staphyloccous aureus
VRE Vancomycin resistant Enterococci spp.
ESBL Extended-spectrum beta (β)-lactamase gram-negative organisms
CRE Carbapenems resistant Enterobacteriaceae
MRAB Multi-resistant Acinetobacter baumannii
The spread of MDROs in health-care settings is common and occurs mostly via health-care workers’ (HCWs) contaminated hands, contaminated items/equipment and environment.
The importance of hand hygiene in preventing health care associated infections (HCAIs) has been long known since the study carried out by Semmelweis in 1884[2]. Many studies down the ages, have repeatedly demonstrated effective hand hygiene to be the single most effective method in reducing HCAIs [3-4].
Despite this, hand hygiene compliance among health care personnel has remained abysmally poor, especially in the intensive care unit (ICU) [5]. This has been attributed in part, due to the poor design and quality of the information and training imparted to health care workers [6–8].
In order to tackle this problem, the World Health Organization (WHO) developed a concept called “My five moments for hand hygiene” [9]. It describes the reference points for hand hygiene and tells the specific moments when hand hygiene is required to effectively interrupt microbial transmission during the normal care of patients.
{kind=link}
There is very little data available on hand hygiene practices among healthcare personnel in India. Thus, we decided to conduct a before–after, prospective, observational study of hand hygiene practices in our ICU, with an interventional strategy based on “my five moments of hand hygiene”
MATERIAL AND METHODS: This observational analytical study was conducted from March 2015 to June 2015 at JIPMER women and children hospital, a tertiary care teaching hospital center in Pondicherry.
Study participants were all healthcare personnel working and visiting in PICU, JIPMER. Health care personnel not willing to give consent for study were only excluded.
Before starting the study verbal consent was taken from all health care personnel in PICU for recording of daily activity. Hand hygiene education module consisted of running of video of hand hygiene daily from 8 am – 9 am in television installed outside PICU. Two weekly classes on hand hygiene and it’s importance in PICU were taken by the principal investigator. Reinforcing the importance of hand hygiene was done in PICU daily bedside. The interventional program targeted resident trainees working/visiting the ICU and all nursing staff working in the ICU.
Posters reinforcing the importance of hand hygiene were already present in PICU. CCTV camera was installed in PICU. CCTV was chosen as a method of surveillance so as to decrease the observer bias in a surveillance done in person by infection control nurse. Also it reduced the human workload and we were able to observe and note observations even during night time.
Whole day activities were recorded in it for whole week. Weekly once the data in memory card of CCTV camera was viewed after dividing each day in 4 blocks of 6 hours. Out of 6 hours in each block, 1 hour period was randomly selected for viewing the video footage. Particulars of any health care personnel were not revealed anywhere. Before the start of the study period, we discussed all aspects of observations in detail regarding what constituted each hand hygiene opportunity and what a lapse is.
Pre intervention data of hand hygiene compliance from January to June 2014 was collected by random observation from infection control nurse. HAI rate data from same period was retrieved from computer based data from PICU desktop where data of all patients is saved.
Hand hygiene compliance rate in health care personnel in JIPMER PICU was 33% (January- June 2014 unpublished data) .In order to raise it to 60% with 95% confidence interval with precision of 5% minimum number of observations required was 369. With 10% attrition rate (due to environmental or mechanical problem) final numbers of observations were 410. Sample size was calculated by using OPENEPI software version 3.03 updated 22/09/2014. Study was conducted over period of 4 months (From march 2015– june 2015). Total number of hours were 2880 (120 x 24), which were divided into equal blocks of 6 hrs making it total 480 blocks . Out of 6 hours block 1 hour was randomly selected, of which video footage viewed. 420 hours of video recording was studied.
Simple random table was used for randomization. Numbers of blocks were numbered from 1-480. Out of which 420 were randomly selected. Out of 6 hours of period in each block, 1 hr period was randomly selected again by simple randomization table by the person not directly involved in study.
Data collection methods including settings and periodicity
Randomly selected 1 hour of video recording in each block of 6 hours was viewed at the end of one week .Number of opportunities of hand hygiene according to ‘My 5 moments of hand hygiene’ [9] were noted. Out of total opportunities number of times hand hygiene was carried out and number of time lapse of opportunity was noted. Observations involving the health care person not giving consent for study were not counted. Rate of hospital acquired infection during this 4 month period was noted. Hospital acquired infection was defined as per standard definition. No blood sampling or any other investigation was done for this study purpose.
STATISTICAL ANALYSIS: Both descriptive and inferential statistics were used to analyze the data. Categorical data was described using frequencies and percentages and compared by using chi square test or Fischer’s exact test. To present the normally distributed data, mean and standard deviation were used and for Non-Gaussian, median was used. Appropriate parametric (Independent students t test) or non-parametric (Mann Whitney U test) were used to compare the groups.
HAI rate before and after are expressed in HAI rate / 1000 PICU days. HAI episodes were divided in VAP and CLABSI. VAP rate was expressed in VAP rate / 1000 ventilation days. CLABSI rate was expressed as rate/ 1000 catheter days.
All tests were two-tailed and a p value of < 0.05 was considered as significant. SPSS 20.0 software (SPSS Inc. Chicago, Illinois) and Epi Info ™ 7 (7.0.9.7, CDC) was used for data analysis.
RESULTS:
Total 420 hours of video footage was viewed.
Total video footage was equally divided in day and night hours. Day was defined as 8 am- 8 pm and night was defined as 8 pm- 8 am.
{kind=link}
Total number of opportunities as per WHO my 5 moments of hand hygiene were 10519. Out of which 5953 were utilized. 4566 opportunities were missed. Overall compliance was 56% .
{kind=link}
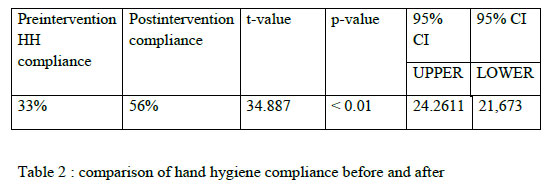
As stated previously, hand hygiene compliance in the same period i.e. Mar 2014 to June 2014 was 33%. Hence we can see that compliance improved from 33% to 56% which is significant with p- value < 0.01
{kind=link}
{kind=link}
As we can see highest compliance was in consultant followed by nursing staff followed by residents but which differed significantly.
As study was conducted over a period of 4 months, month wise HH compliance also studied which showed highest compliance in June followed by April. Least compliance was found in month of March which was significantly less compared to April, May, and June. This can be attributed to the reason that study commenced in month of March with intervention to improve compliance also started in March showing it’s positive effect in subsequent months.
{kind=link}
HH compliance also differed according to ‘5 moments of hand hygiene’ of WHO campaign in a way shown following chart.
{kind=link}
HH compliance was highest before aseptic task, 88.76% followed by “before contact with patient” , 64.73%. Least compliance was seen with “after contact with patient surrounding”, 28.11%.
HH compliance also differed according to shift of the work as in day or night. In the morning hours which were defined as 8 am to 8 pm and night hours defined as 8 pm -8 am. Compliance was significantly less in night hours with mean of 57.36% in morning hours while 54.56 in night hours with p-value < 0.05.
{kind=link}
Ventilator associated pneumonia (VAP) rate between march 2014 – June 2014 was 22.3/1000 ventilation days. Central line associated blood stream infection ( CLABSI) during the same period was 10.06/ 1000 catheter days( unpublished data). In intervention phase i.e. march 2015 to jun 2015, there was significant fall in VAP rate which was 13.42/ 1000 ventilator days, and CLABSI rate which was 2.78/1000 catheter days.
Discussion : We in our institution, routinely use chlorhexidine based hand rub for hand hygiene required in “my 5 moments of Hand hygiene”. This evidence-based, field-tested, user-centred approach is designed to be easy to learn, logical and applicable in a wide range of settings [9].
We used video surveillance for monitoring of hand hygiene compliance as per these 5 moments of hand hygiene as used previously by Armellino et al [10]. Total 420 hours of video recording was viewed which was equally divided in day and night shift to see the diurnal variation in hand hygiene compliance. Total opportunities for HH observed during video surveillance were 10519, out of which 5953 opportunities were used with total compliance of 56% which was comparable o previous studies by Mathai et al and Salem et al [11,12]. This was the post intervention data. In study by Salem et al hand hygiene compliance increased from 42.9% pre-intervention to 61.4% post-intervention, P < 0.001 with similar intervention. In another study by Mathai et al hand hygiene compliance improved significantly to 56% after intervention to improve hand hygiene.
The intervention which we used to increase HH compliance i.e. biweekly classes , bedside reinforcement of hand hygiene importance, similar intervention was used by Mathai et al [11].
In our study HH compliance was maximum in “before aseptic task” 88.76 % , followed by “ before contact with patient” 64.73%. This was opposite to result seen by Mahfauz et al in which before contact with patient was significant risk factors for hand hygiene non-compliance in the hospital [13].Least compliance in present study was with “ after contact with patient surrounding” 28.11%.
Compliance among health care personnel according to their work rank differed significantly. Highest compliance was noticed in PICU consultant with 98.5%. This was differing with previous studies by Mahfauz et al [13]. In study by Mahfauz et al being a physician was significant risk factor for hand hygiene non-compliance in the hospital [13].
Compliance was highest among nurses after consultant (77.25%) while in residents it was 52.25%. Results were similar to previous observations by Mathai et al, Salem et al and Victor et al [11,12,14].
This can be contributed to fact that residents have tighter schedule and more mental stress. This fact tells us that we need to focus on residents more for hand hygiene compliance and give them positive feedback of improved compliance frequently as residents and nurses are the personnel who will be in contact with patients for longest duration.
There was significant fall in HAI in the post intervention period as rate of fall in HAI has already been told in results This can be attributed to increase in hand hygiene compliance significantly as rest of the factors which can affect HAI rate i.e. profile of patient admitted, nurse to patient ratio, doctor to patient ratio was also similar. Similar results were seen by Salama et al. in his study, the rate of overall health care-associated infections/1000 patient-days, fell from 37.2 pre-intervention to 15.1 post-intervention (P < 0.001); the rate of bloodstream infections, which fell from 18.6 to 3.4/1000 central-line-days (P<0.001); and the rate of lower respiratory tract infections, which fell from 17.6 to 5.2/1000 ventilator-days (P<0.001) [12].
In present study, we were able to see diurnal variation in hand hygiene compliance as have been previously reported. Compliance during day hours was significantly more than night hours 57.36% and 54.56% with a p-value <0.05. Similar observation has been made previously by Sahay et. al. in his study, hand hygiene compliance dropped during the night for doctors (81% vs 46%, respectively, P < .001), for nurses (64% vs 55%, respectively, P = .02), and for paramedical staff (44% vs 31%, respectively, P = .01). This again emphasizes importance of repeated reinforcement of importance of hand hygiene compliance [15].
The HH compliance in duration of 4 months was least in month of March, 46.43 %, while highest in June and April (64.45 and 63.87 % respectively.
Significance of this can be seen as there was not a single c/o of HAI in the form of VAP and CLABSI was noted in the month of April., while in the month of March there were 3 events of VAP and 1 CLABSI amounting to VAP rate of 13.57/ 1000 ventilator days and CLABSI rate of 5.95/ 1000 catheter days. While most of the other factors affecting the occurrence of HAI were same in both months, though not correlated systematically.
Limitations of study:
1) Method of collection data of hand hygiene compliance before and after intervention was not same.
2) Other factors which might decrease incidence of HAI apart from hand hygiene compliance were not formally studied.
CONCLUSIONS: 1) It can be concluded that rate of hand hygiene compliance can be increased significantly by reinforcing its importance repeatedly to medical staff working in I.C.U.s.
2)Increase in hand hygiene compliance can decrease the number of rate of hospital acquired infections
DECLARATIONS:
Contributors: R. Rameshkumar -Conceptualization ,analysis of the collected data and preparation of manuscript. Jayanta Vagha-Study design and Methodology. Sham B. Lohiya-Literature search, collection of data and revision of the manuscript.
Competing and conflict of interests: None
Funding– None
REFERENCES:
1. .The evolving threat of antimicrobial resistance Options for action. Available World Health Organization (2012b) at: http://www.who.int/patientsafety/implementation/amr/publication/en
2. Pittet D, Boyce JM. Hand hygiene and patient care: Pursuing the Semmelweis legacy. Lancet Infect Dis. 2001; 1: 9–20.
3. Didier Pittet, MD, MS; Sir Liam Donaldson, MD, MSc. Clean Care is Safer Care: The First Global Challenge of the WHO World Alliance for Patient Safety. Infect Control Hosp Epidemiol. 2005;26(11): 891-2
4. Rosenthal VD, Maki DG, Mehta A, Alvarez-Moreno C, Leblebicioglu H, Higuera F et al. International Nosocomial Infection Control Consortium report, data summary for 2002-2007. Am J Infect Control. 2008; 36: 627–37.
5. Kretzer EK, Larson EL. Behavioral interventions to improve infection control practices. Am J Infect Control. 1998; 26: 245–53.
6. Vicente KJ. What does it take? A case study of radical change toward patient safety. Jt Comm J Qual Saf. 2003; 29: 598–609.
7. Lin L, Vicente KJ, Doyle DJ. Patient safety, potential adverse drug events, and medical device design: A human factors engineering approach. J Biomed Inform.2001; 34: 274–84.
8. Leape LL, Woods DD, Hatlie MJ, Kizer KW, Schroeder SA, Lundberg GD. Promoting patient safety by preventing medical error. J Am Med Assoc. 1998; 280: 1444–7.
9. Sax H, Allegranzi B, Uc¸kay I, Larson E, Boyce J, Pittet D. My five moments for hand hygiene: A user-centred design approach to understand, train, monitor and report hand hygiene. J Hosp Infect. 2007; 67: 9–21.
10. Armellino D, Hussain E, Schilling ME, Senicola W, Eichorn A, Dlugacz Y et al. Using high-technology to enforce low-technology safety measures: the use of third party remote video auditing and real-time feedback in health care. Clin Infect Dis 2011;54:1-7.
11. Ashu S. Mathai, Smitha E. George, John Abraham. Efficacy of a multimodal intervention strategy in improving hand hygiene compliance in a tertiary level intensive care unit Indian J Crit Care Med. 2011; 15(1): 6–15.
12. Salama MF1, Jamal WY, Mousa HA, Al-Abdulghani KA, Rotimi VO. The effect of hand hygiene compliance on hospital-acquired infections in an ICU setting in a Kuwaiti teaching hospital. J Infect Public Health. 2013; 6(1): 27-34
13. Ahmed A. Mahfouz , Mohammad N, El Gamal b, Tarik A, Al-Azraqi. Hand hygiene non-compliance among intensive care unit health care workers in Aseer Central Hospital, south-western Saudi Arabia ,Int J Infect Dis, 2013;17: e729–e32
14. Victor D. Rosenthal, MD, MSc, CIC, Mandakini Pawar, MD, Hakan Leblebicioglu, MD, Josephine Anne Navoa-Ng, MD, Wilmer Villamil-Gómez, MD, Alberto Armas-Ruiz, MD Impact of the International Nosocomial Infection Control Consortium (INICC) Multidimensional Hand Hygiene Approach Over 13 Years in 51 Cities of 19 Limited-resource Countries From Latin America, Asia, the Middle East, and Europe Infect Control Hosp Epidemiol. 2013;34(4):415-423.
15. Sahay S Panja S Ray S Rao BK Diurnal variation in hand hygiene compliance in a tertiary level multidisciplinary intensive care unit. Am J Infect Control. 2010 Sep;38(7):535-9.
Issue: January-March 2019 [Volume 8.1]