Corresponding Author: Dr. Sachin Damke, Professor & Head Department of Paediatrics, JNMC, Acharya Vinoba Bhave Rural Hospital, Sawangi, Wardha, Maharashtra, India
RECEIVED : 12 th October,2018 ; REVIEWED: 24th December,2018 ; ACCEPTED :23 th January 2019.
Abstract: Assisted ventilation has become an indispensable part of the neonatal intensive care. It is helpful to reduce the high mortality in this group of neonates and identification of risk factors is important.
Objectives: To assess the current status of neonatal ventilation in a tertiary care neonatal unit in a rural hospital in central India, to identify the common indications for ventilation, analyze the complications that arise, and evaluate the short term outcome as measured by survival.
Design: Hospital based prospective observational study
Setting and participants: conducted on neonates who required mechanical ventilation over period of 2 years (1st September 2015 – 31st August 2017).
Materials and methods: Neonates requiring mechanical ventilation during the study period of 2 years (1st September 2015 – 31st August 2017) were enrolled in the study.
Neonates who received mechanical ventilation for minimum of 6 hours during the study period were included in the study after written informed consent from parents. Babies who expired within 6 hours of life, neonates with birth weight < 500 grams, abrupt termination of ventilator support for any reason and gestational age <26 weeks were excluded.
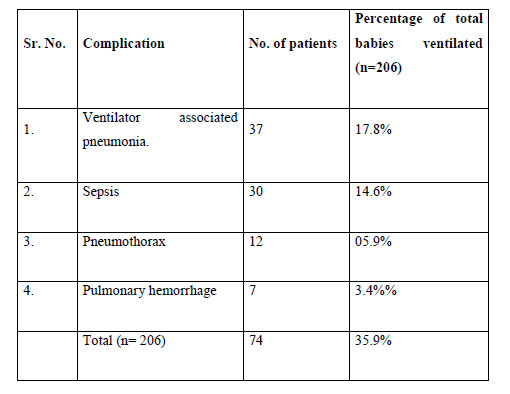
Results: 206 neonates were included in the study. Males comprised of 56.8% of ventilated neonates. The most common indication of ventilation was birth asphyxia, in 29.1% neonates, followed by neonatal sepsis (22.3%), respiratory distress syndrome (18.4%), and meconium aspiration syndrome (13.1%). Complications were seen in 35.9% neonates, the most common complication was ventilator associated pneumonia (50%), sepsis (40.5%), pneumothorax (16.2%). Survival rate among the ventilated neonates was 45.6%.
Conclusion: Neonates with birth asphyxia and sepsis were the major problems in NICU, which must be addressed to improve outcome.
KEYWORDS: Neonates, mechanical ventilation
INTRODUCTION: Neonatal deaths account for nearly 64% of all infant deaths and 50% of under-five mortality in India. Birth asphyxia, congenital pneumonia, immaturity, hyaline membrane disease, intraventricular haemorrhage, and neonatal infections are leading causes of neonatal mortality in our country (1). Many critically sick babies, who develop life-threatening apnoea or cardiovascular collapse from a variety of causes, need cardiopulmonary resuscitation(2,3). Assisted ventilation has become an indispensable part of the neonatal intensive care(1). Infants with progressive respiratory distress with impending respiratory failure can be supported and saved by assisted ventilation facilities(2,3).
Since its introduction into the modern ICUs, mechanical ventilation has undergone continuous evolution. Epidemiologic and environmental factors in the ICU are important to critical care because they can affect care and mortality(4,5).
OBJECTIVES: To assess the current status of neonatal ventilation in a tertiary care neonatal unit in a rural hospital in central India, to identify the common indications for ventilation, analyze the complications that arise, and evaluate the short term outcome as measured by survival.
Design: Hospital based prospective observational study
Setting and participants: Conducted on neonates who required mechanical ventilation over period of 2 years (1st September 2015 – 31st August 2017).
MATERIAL AND METHODS: This prospective observational study was conducted in a tertiary care hospital, attached to a medical college and neonates requiring mechanical ventilation during the study period of 2 years (1st September 2015 – 31st August 2017) were enrolled in the study.
Neonates who received mechanical ventilation for minimum of 6 hours during the study period were included in the study after written informed consent from parents. Babies who expired within 6 hours of life, neonates with birth weight < 500 grams, abrupt termination of ventilator support for any reason and gestational age <26 weeks were excluded.
The babies were managed as per prevailing protocol. The required data was obtained and entered in a predesigned validated proforma.
Statistical analysis: The results obtained were tabulated and analysed and using the chi square test and multiple logistic regression, p value was calculated. The results were tested at 5% level of significance.
OBSERVATION & RESULTS: We included 206 neonates who were mechanically ventilated and fulfilled the inclusion criteria. Of these, males were 117 (56.8%) and females were 89 (43.2%). 96 (46.6%) neonates were full term and 110 (53.4%) were preterm. 50 neonates (24.3%) had normal weight i.e. >2.5kg; while 156 (75.7%) were low birth weight babies (Table 1)
{kind=link}
The common indications of ventilation observed are given in table 2, the most common being birth asphyxia, reported in 62 neonates (30.1%). Of the 40 neonates with RDS, 26 were male (65%) while 14 were females (35%).
Table 2: Indication (cause) of ventilation:
{kind=link}
{kind=link}
Ventilator parameters between survivors and non-survivors were compared in this study. Less ventilator pressures were required among the group of survivors while the requirement of pressures and the other ventilatory settings were increased among those of non-survivors (Table 3). Ninety four (43.6%) neonates were successfully weaned; SIMV with PS was the preferred mode in 53 (56.4%) neonates. Complications were seen in 74 (35.9%) neonates, the most common being ventilator associated pneumonia (Table 4)
Table 4: Neonates with complications of mechanical ventilation:
{kind=link}
Out of total 206 neonates, we could salvage 94 neonates (45.6%). Of the 39 ELBW babies, only 5 neonates (12.8%) could be salvaged, whereas of the 50 normal birth weight babies, 32 could be salvaged (64%). Thus survival rate is fairly rising with increasing weight of the neonate.
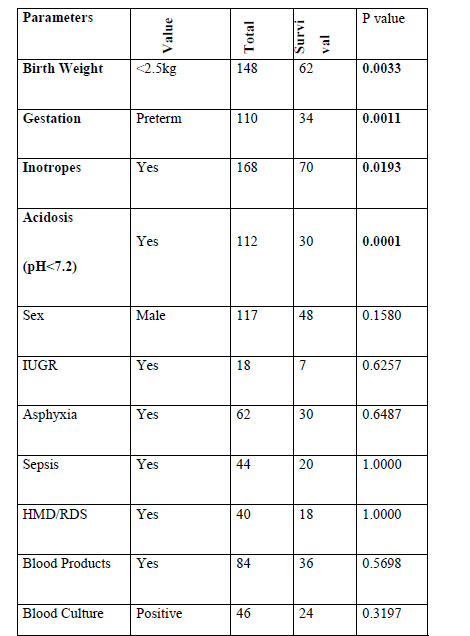
Table 5: Predictors of survival:
{kind=link}
Using logistic regression, the predictors of survival were birth weight >2.5kg, term gestation, ventilated babies not requiring inotropes and acidosis with ph<7.2.
DISCUSSION: Assisted ventilation is one of the most important advancement in neonatal medicine which has reduced neonatal mortality considerably. Shah et al(6) 2013 conducted a similar study in eastern Nepal, and found that birth asphyxia (34%) and sepsis (30.8%), were the most common indications as seen in our study. Mannan et al also concluded asphyxia as the most common indication. While Srinivas et al(7) conducted a retrospective study at Mangalore and found that, respiratory distress syndrome and neonatal sepsis were the most common indications for ventilation. Similarly, Krishnan et al concluded sepsis as the most common indication.
In a study done by Acharya et al(8) in tertiary care hospital, Hyderabad, septicemia was the most common complication, followed by air leak, tube block and weaning failure.
Maiyya et al(9) and Mannan et al(10) had VAP as the most common complications as seen in present study. While Prabha et al(11), Bhatt et al(12), and Singh et al(13) and Mathur et al(14) had sepsis as their most common complications. In the study by Jahan et al(15) at Bangladesh,, pneumonia & pneumothorax were the common complications of mechanical ventilation followed by neonatal sepsis and pulmonary hemorrhage.
Similar to our study, Sangita et al(16) conducted a study at Surat andhad higher mortality. Similarly, Srinivas et al(7) Iqbal et al(17), Singh et al(13), also had higher mortalities. Most of the studies had heigher mortality, however, Hossain et al(18) and Mathur et al(14) had 29.4% and 26% mortality respectively.
In our study, the factors such as weight <2.5kg, prematurity and acidosis (ph<7.2), significantly affected the outcome of neonates. In the study done by Acharya et al(8), no significant association was observed between birth weight or gestational age and survival rates. He also observed that survival was highest for neonates ventilated for hyaline membrane disease (34.3%), followed by meconium aspiration (17.1%). In the study by Iqbal et al(17), apnea and sepsis significantly affected the outcome of the patient. In a study done in Eastern U.P(20)., it was observed that survival was worst in babies weighing< 1.5 kg(40%) and those < 32 wk of gestation(36%).
CONCLUSION: Majority of the neonates on mechanical ventilator were secondary to birth Asphyxia, neonatal sepsis, respiratory distress syndrome and meconium aspiration syndrome. Complications during the course of mechanical ventilation included ventilator associated pneumonia, sepsis, pneumothorax and atelectasis. Survival rate of the neonates who were mechanically ventilated was 45.6%.Most common weaning mode used in this study was SIMV with pressure support, followed CPAP with pressure support.
DECLARATIONS:
Contributors: – Sachin Damke – Determination of study design and methodology, Prajakta Dekat -collection of data e analysis of the collected data, literature search and preparation of manuscript. Revat Meshram– Conceptualization, and revision of the manuscript
Competing and conflict of interests: None
Funding- None
REFERENCES:
1. Meharban Singh. The Current status and Challenges of Perinatal Services in India. Care of the Newborn, Sixth edition August 2004; 2: 12-19.
2. Clinical profile of mechanically ventilated newborns at tertiary care level hospital. Bhatt S, Nayak U, Agrawal P, Patel K, Desai D.
3. Trivedi SS, Chudasama RK, Srivastava A. Study of Early Predictors of Fatality in Mechanically Ventilated Neonates in NICU. Online J Health Allied Sci South India. 2009;8(3):1-4.
4. Halm EA, Lee C, Chassin MR. Is volume related to outcome in health care? A systematic review and methodologic critique of the literature. Ann Intern Med 2002; 137: 511-20.
5. Kahn JM, et al. Hospital volume and the outcomes of mechanical ventilation. N Engl J Med 2006; 355: 41-50
6. Shah BK, Shah GS, Mishra OP. Mechanical Ventilation in Neonates: Experience at a Tertiary Care Center in Eastern Nepal.
7. Srinivas N, Oommen R, Shriyan A. Neonatal Mechanical Ventilation: Indications and Outcome. IJSR. 2016 June ; 5(6)
8. Acharya A, Sastry CPVR, Kulkarni SR. Experiences Of Neonatal Mechanical Ventillation In Tertiary Care Hospital, Hyderabad. Intrl J Pharmaceutical and Medical R. Feb 2015;3:(1):15-23
9. Maiya PP, Vishwanath D, Hegde S, Srinivas TP, Shantala CC, Umakumaran P, Naveen B, Hegde RK. Mechanical Ventilation Of New Borns: Experience From A Lev El Ii Nicu.
10. Mannan MA, Jahan N, Iqbal S, Ferdous N, Dey S, Farhana T, Nazma N. Short Term Outcome of Preterm Neonates Required Mechanical Ventilation. ChattagramMaa-O-Shishu Hospital Medical College Journal. 2017 Mar 6;15(2):9-13.
11. Nayana PP, Somasekharan PK, Junaid RM. Outcome of ventilation in hyaline membrane disease: the Indian Experience. Journal of Evolution of Medical and Dental Sciences. 2016 Jun 30;5(52):3378-82.
12. Bhatt S, Nayak U, Agrawal P, Patel K, Desai D. Clinical profile of mechanically ventilated newborns at tertiary care level hospital. Int J Res Med. 2015;4(2):86-90.
13. Singh M, Deorari AK, Paul VK, Mittal M, Shanker S, Munshi U, Jain Y. Three-year experience with neonatal ventilation from a tertiary care hospital in Delhi. Indian pediatrics. 1993 Jun 1;30(6):783-9.
14. Mathur NB, Garg P, Mishra TK. Predictors of fatality in neonates requiring mechanical ventilation. Indian pediatrics. 2005 Jul 1;42(7):645.
15. Jahan N, Haque ZS, Mannan MA, Nasrin M, Afroz F, Parvez A, Rahman T, Islam M. Indication and short term outcome of Mechanical Ventilation in Neonates in a tertiary care hospital. Bangladesh Journal of Medical Science. 2017 Jan 16;16(1):24-8.
16. Sangeeta ST, Rajesh KC, Anurakti S. Study of early predictors of fatality in mechanically ventilated neonates in NICU. Online J Health Allied Sci2009;8:3-9. Available from: URL: http://www.ojhas.org/ issue31/2009-3-9.
17. Iqbal Q, Younus MM, Ahmed A, Ahmad I, Iqbal J, Charoo BA, Ali SW. Neonatal mechanical ventilation: indications and outcome. Indian journal of critical care medicine: peer-reviewed, official publication of Indian Society of Critical Care Medicine. 2015 Sep;19(9):523.
18. Hossain MM, Shirin M, Al Mamun MA, Hasan MN, Sahidullah M. Predictors of mortality in ventilated neonates in intensive care unit. Bangladesh Journal of Child Health. 2009;33(3):77-82.
19. Rai R, Singh DK. An experience with neonatal ventilation in eastern UP. Indian journal of pediatrics. 2009 Nov 1;76(11):1177
Issue: January-March 2019 [Volume 8.1]