A Study on Demographic & Radiological Profile of Children with Seizure Disorder Admitted in the Pediatric Emergency Ward of a Tertiary Care Centre
ORIGINAL RESEARCH
Corresponding author: Dr. Mrinalkanti Ghosh*, Associate professor, Department of Radiodiagnosis, Burdwan Medical College
Satabdibag 2nd lane , Sripally Purba-Barddhaman,West Bengal-713103,
Mob No: 9434014968,Email: drmkghosh@outlook.com
Received:23 th August,2018 Reviewed:24th October 2018, Accepted:21 th December 2018
Citation Of Atricle: Taraknath Ghosh, Mrinalkanti Ghosh, Kamirul Islam, Soutrik Seth, Atanu Roy, A K Datta A Study On Demographic & Radiological Profile Of Children With Seizure Disorder Admitted In The Pediatric Emergency Ward Of A Tertiary Care Centre; New Indian Journal Of Pediatrics 7:4
ORIGINAL RESEARCH
![]()
ABSTRACT: Background & Objectives: Seizure disorder is one of the common neurological problems of children. We conducted this study to find out the common clinical presentations & radiological features of seizure disorder.
Methods: It was a hospital-based prospective study conducted among all the children presented with seizure disorder in the pediatric emergency department of Burdwan Medical College between January 2013 to December 2016. Complete enumeration methods was followed to identify 796 subjects. All the statistical analysis was done by SPSS software versio 19.0.
Results: The study includes 796 subjects with a mean age of 5.7±2.1 years.We noticed that GTCS is more common among lower aged male children of rural area whereas partial seizure is more common among elderly female children of urban area. Ring enhancing lesion is the most common radiological findings of partial seizure but hypoxic ischemic encephalopathy/structural abnormality of brain was the leading cause of GTCS.
Conclusion: The study reflects the profile of patients with seizure disorder in a rural tertiary care centre. Further multi-centric studies should be undertaken.
Keywords: seizure disorder,Ring enhancing lesion hypoxic ischemic encephalopathy,structural abnormality
INTRODUCTION: Seizure disorder affects 50 million people worldwide & 80% of them belonged to developing countries.1,2 Children are of no exception. Though Febrile seizure is the most common cause of seizure in children, it may be associated with grave diseases like infection, structural abnormalities of brain etc. Apart from febrile seizure birth asphyxia, metabolic cause, structural abnormalities of brain are important causes of seizure.3,4,5 Seizure disorder leads to more than 7 million DALYs. Incidence of epilepsy in India is 27.3 per 100000 population.6 Properdiagnosis of seizure disorder is always challenging in developing countries where resource is limited. Neuro-imaging emereged as an important modality of diagnosing seizure disorder now a days.7,8,9
METHODS: One hospital (in-patient)- based prospective study was conducted among children (≤12 years) admitted with convulsion disorder in the Pediatric Emergency Ward of Burdwan Medical College, a rural tertiary care centre in between January, 2013 to December, 2016. All patient admitted with convulsion disorder in the specified time period were selected for the study & complete enumeration methods is thus followed. Children who were previously diagnosed as neurological diseases, which were seriously ill to undergo a neuroimaging procedure or whose parents were not willing to give consent were excluded from the study. 844 children were admitted with a clinical diagnosis of convulsion disorder in the study period & 48 children were excluded from the study (2 for not giving consent, 32 children were previously diagnosed as static encephalopathy & 14 children were died before any neuro-imaging procedure). So, the study population came to be 796. Data were collected by using a pre-designed pre-tested semi-structured schedule. Physical examination was done by same investigator in all cases which is confirmed by other investigators. Every CT/MRI plates were checked by two different radiologists. Prior ethical clearance was taken.[BMC/PG/194/1(1)]
Operational Definition: Seizure is defined as synchronous neuronal discharge of neurons leading to motor activity.10 Seizure disorder is defined as two or more episodes of recurrent unprovoked seizure.10
Statistical Analysis: Collected data were entered into Microsoft Office Excel Worksheet after double-checking. Continuous data were expressed in the terms of mean & standard deviation,whereas proportions were used for categorical variable. Chi-square test & Student’s t test were used to check the difference between categorical data & continuous data, respectively. All the analysis was done by SPSS version 19.0 (Statistical package for social sciences). All the data were rounded to one decimal point. P<0.05 was taken as statistically significant.
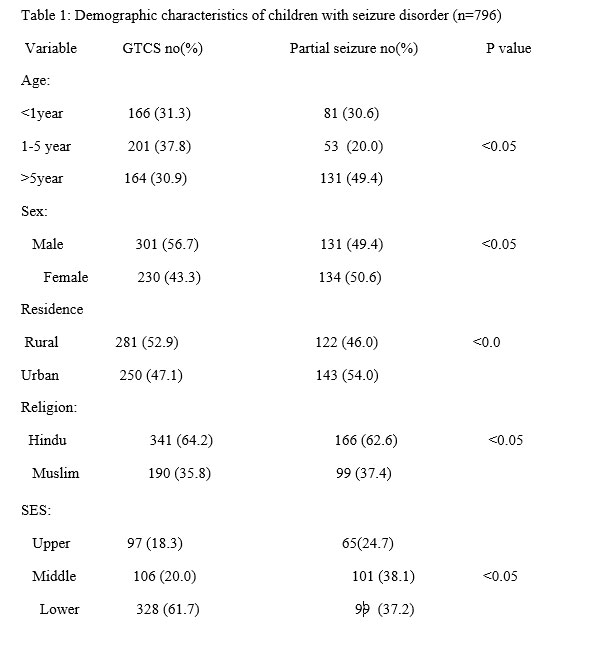
RESULTS: The study includes 796 subjects with a mean age of 5.7±2.1 years. Majority of them belonged to 1-5 years age group, were male, were from rural area, were Hindu & belonged to lower socio economic status.
GTCS was more common among children of 1-5 year age group, male children, and children of rural area, Hindu children and children of lower socioeconomic status. Partial seizure was more prevalent of children >5 year age group, females, urban children, Hindu children & children of middle socioeconomic status.
Common associated clinical features with GTCS were fever, alteration of sensorium & vomiting. On the other hand, movement disorder, alteration of sensorium & focal neurological signs were more prevalent among children with partial seizure.
Normal CT/MRI was most common among both GTCS & partial seizure group. Among abnormal findings, ring enhancing lesion was most common among children with partial seizure followed by intracranial space-occupying lesions. Among GTCS, changes due to hypoxic ischemic encephalopathy & structural brain abnormalities were most common.
All these findings are statistically significant.
Discussion: In our study we found that seizure disorder is more common among male children & children of middle age group. The finding is partially similar to the findings of Adhikari S11 et al & Sarvanan S12 et al from Nepal & southern part of India respectively. Similar to us they also noted seizure disorder is more common among males, but contrary to our findings they observed that seizure disorder is more common among the children of younger age group. Similar to the observations of Chen CY13 et al, we also noted that GTCS is more prevalent among patients of children. Sarvanan S et al also noted the same. Major clinical features in our study were fever, altered sensorium & vomiting. Sarvanan S et al also noted the same in their study. Similar to the observations of Ojha AR14, fever is present in maximum cases of GTCS. Adhikari S11 et al & Srestha S15 et al found that NCC was the leading neuro-imaging features of children with seizure disorder. Contrary to them we found normal CT/MRI is more common among patient with seizure disorder. Though among abnormal CT/MRI ring enhancing lesion is most common cause of partial seizure but hypoxic ischemic encephalopathic changes are most common among children with GTCS.
CONCLUSION: We noticed that GTCS is more common among lower aged male children of rural area whereas partial seizure is more common among elderly female children of urban area. Ring enhancing lesion is the most common radiological findings of partial seizure but hypoxic ischemic encephalopathy/structural abnormality of brain was the leading cause of GTCS. The main limitations of this study are that it is a cross-sectional study and excludes neonate. These may alter the findings of this study significantly. But this study is able to give significant information regarding demographic profile of children with seizure disorder in rural area. This study may further help to form treatment protocol of seizure disorder. But further studies preferably multicentric will have to be conducted for better information.
DECLARATIONS: Contribution of authors: Mrinalkanti Ghosh -concept ,strategy, Taraknath Ghosh, – supervision andrevision of manuscript, A K Datta –guidance, Kamirul Islam, -data collection,statistical analysis, Soutrik Seth – data collection,initial manuscript, , , Atanu Roy- statistical analysis initial manuscript
Funding: None
Conflict of interest: None
Ethical approval: Approved by hospital ethical committee
References:
- Vining EP. Pediatric seizures. Emergency Medicine Clinics of North America.1994; 12: 973–88.
- Singhi P, Singhi S. Neurocysticercosis in children. Indian Journal of Pediatrics.2009; 76: 537–45.
- McAbee GN, Wark JE. A practical approach to uncomplicated seizures in children. American family Physician. 2000;62 :1109–16,.
- Rajbhandari KC. Epilepsy in Nepal. Canadian Journal of Neurological Sciences.2000;31: 257–60.
- Stafstrom CE. Neonatal seizures. Pediatrics in Review.1995;16:248–56.
- Idro R, Gwer S, Kahindi M. The incidence, aetiology and outcome of acute seizures in children admitted to a rural Kenyan district hospital. BMC Pediatrics. 2008; 8: 1.
- Murthy JMK, Yangala R. Acute symptomatic seizures – Incidence and etiological spectrum: A hospital-based study from South India. Seizure. 1999;8: 162-5.
- Rayamajhi A, Singh R, Prasad R, Khanal B, Singhi S: Study of Japanese encephalitis and other viral encephalitis in Nepali children. Pediatrics International Official Journal Japan Pediatric Society. 2007; 49: 978–84.
- Huang CC, Chang YC, Wang ST. Acute symptomatic seizure disorders in young children – a population study in southern Taiwan. Epilepsia. 1998;39: 960–4.
- Hauser WA, Kurland LT. The epidemiology of epilepsy in Rochester, Minnesota, 1935 through 1967. Epilepsia. 1975;16:1–66.
- . Adhikari S, Sathian B, Koirala DP, Rao KS: Profile of children admitted with seizures in a tertiary care hospital of Western Nepal. BMC Pediatrics. 2013;13:1.
- Saravanan S. Profile of children admitted with seizures in a tertiary care hospital in South India. IOSR Journal of Dental and Medical Sciences. 2013; 4: 56–61.
- Ojha AR, Aryal UR. Clinico-etiological profile of children with seizures admitted in a tertiary centre. Journal of Kathmandu Medical College. 2015; 4:55–58.
- Chen CY, Chang YJ, Wu HP. New-onset seizures in pediatric emergency.Pediatrics and Neonatology. 2010;51:103–11.
- Shrestha BM. Childhood neurocysticercosis: clinico-radiological profile and outcome. Journal of Nepal Paediatric Society.2008; 28:14–16.


Issue: October-December 2018 [Volume 7.4]