Role of imaging in etiological diagnosis of childhood seizures – age group 1 month to 5 years
Original Research
Original Research
![]()
Abstract:
Background: Seizure is the manifestation of abnormal brain electrical activity that causes momentary alteration of behavior and consciousness. Thus in this present study, the etiology of childhood seizures has been established with the help of structural neuro-imaging.
Methods: The Case-Control Study was performed on 96 children of age group 1 month – 5 years presenting with seizures in the Pediatric department of Institute Of Child Health, Kolkata for a period of one and a half years.
Results: The study showed 23 out of 96 cases (42.59%) had seizures due to an infectious etiology. 11 out of 96 cases (20.37 %) suffered seizures because of developmental/ congenital brain lesions. Perinatal causes ranked next highest (12.96%)
Conclusions: we have established that neuroimaging specially MRI had an incredible role to play in the etiological diagnosis of childhood seizures. There was a strong association between positive neurological signs and symptomatic seizure.
Key words: seizure, epilepsy, developmental delay, neuroimaging
Introduction:
Seizure is the manifestation of abnormal brain electrical activity that causes momentary alteration of behavior and consciousness. “Epilepsy” is derived from a Greek word meaning “to seize upon” and is synonymous with recurrent seizure disorder – by Douglas R.Nordli, JR.MD.(1) Recent works of Nordli have shown that in the majority of children, a single seizure is not a harbinger of epilepsy. Instead, these children with single isolated seizure are a result of an acute disturbance of brain function rather than the manifestation of a persistent underlying pathologic process. Epidemiologic studies have shown certain postnatal insults like birth trauma, CNS infection, cerebrovascular accidents and brain tumours greatly increase the incidence of childhood epilepsy. Although convincing evidence attributes some cases to specific etiologies, the cause of 70 % of all cases of seizures is unknown.(2)Hence, besides a careful and detailed history, a minimal work up of a seizure includes an EEG (electroencephalography), estimation of blood parameters, electrolytes and CSF examination.(3) The role of neuro-imaging in the investigation of seizures is challenging. The basic aim is to record on a film (or display on a monitor) a pattern of densities (or illumination level on the monitor) that corresponds to and conveys diagnostic information about the size, shape and distribution of the abnormality in the brain tissue.(4) The field of neuro-radiology has become a fast moving, demanding and exciting multi disciplinary activity.(5) It comprises of both structural and functional neuro-imaging. Structural brain imaging includes Ultrasonography, C.T. Scan and Magnetic Resonance Imaging and Functional neuro-imaging comprising of f-MRI, PET, SPECT AND MR- Spectroscopy.(6) Thus in this present study, the etiology of childhood seizures has been established with the help of structural neuroimaging.
Aims and objectives:
- To establish the etiological diagnosis of childhood seizures by neuro-imaging and to establish percentage incidence of the different causes of seizures.
- Age specific incidence and causes of seizures.
- To delineate the causal association of risk factors of childhood seizures.
Methods:
This case-control study was conducted in children between 1 month to 5 years of age admitted with seizure at Institute Of Child Health, Kolkata from July 2014 to December 2015. Children presenting with seizures have been collected randomly from the indoor admission in ICH. Neonatal seizure and typical febrile seizure are excluded from the study. First, detailed history was taken with description from eyewitness to rule out Non-epileptic seizure disorder followed by neurologic and other systemic examinations. Then routine investigations were followed, based on the presenting features, e.g. CSF and blood to rule out infective etiology in children presenting with fever.(7). Only Structural neuro-imaging have been included in the study, which include USG, CT Scan and MRI. Because of non-availability and nonaffordability, functional neuro-imaging namely PET, SPECT and NMR spectroscopy has been excluded from the study.
EEG was conducted in almost all patients to detect seizure type or to locate any lateralizing signs. Demonstration of paroxysmal discharge on the EEG is diagnostic of epilepsy but a normal EEG does not preclude the diagnosis of epilepsy because inter-ictal recording is normal is approximately 40% of patients.(3) Activation procedures, e.g. hyperventilation, eye closure, photic stimulation and when indicated sleep deprivation and special electrode placement were performed to increase the positive yield.(3) Then the patients underwent neuroimaging depending on age, suspicion from history, availability and affordability. Ultrasonographywas the primary investigative procedure for infants, performed through the anterior fontanelle which is available as an acoustic window. Anterior fontanelle closure began at about 9 months of age and is usually complete by 15 months of age.(8) Images are obtained in both coronal and sagital planes.
CT SCAN was done in infants and young children of the study.Sedation were given because lack of head movement was essential. Intravenous injection of radiographic contrast was given when indicated.
MRI brain was performed in the study population and following things were noted:
- T1 weighted images to evaluate anatomy.
- Fluid attenuated inversion recovery (FLAIR) and T2 weighted images for pathologic changes.
- T1 weighted images with gadolinium contrast images when evaluating a lesion (e.g. Neoplasm, infarction, infection or vascular anomalies).
- Diffusion weighted images for acute infarct, oedema and injury.
- Finally, the positive yield has been compared and expressed graphically.
Results:
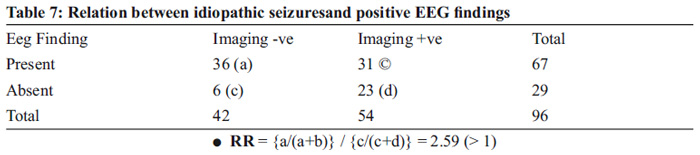
The Case-Control Study was performed on 96 children of age group 1 month –5 years presenting with seizuresin the Pediatric department of Institute Of Child Health, Kolkata for a period of one and a half years (July 2014 to December2015). EEG was done in all cases to confirm a seizure activity and to rule out non-epileptiform seizures. Each of the children underwent some Imaging (USG, CT Scan, MRI) or the other, or a combination of two for a better yield. Out of 96 cases, 54 had positive findings in imaging i.e. 56.25% cases had symptomatic seizures and 42 had no positive yield through imaging i.e. 43.75% cases had idiopathic seizures (Table 1). Male : Female = 1.74 : 1, means male preponderance existed. Idiopathic seizures were more common in males. Highest incidence of childhood seizures was found in the 2nd year of life. Idiopathic seizures were more common in the 2nd year and symptomatic seizures were more common in the 1st year. The study showed 23 out of 96 cases (42.59%) had seizures due to an infectious etiology, which meant infective causes of seizures were highest in our country.11 out of 96 cases (20.37 %) suffered seizures because of developmental/ congenital brain lesions. Perinatal causes ranked next highest (12.96%) (Table 3).Generalized tonic clonic seizures were found in 47 out of 96 cases (48.95%). Focal seizures were found in 37 out of 96 cases (38.54%), the next most common presentation (Table 4).There was a strong association between positive neurological signs and symptomatic seizures (RR=3.4) in the study (Table 5).Temporal association existed between idiopathic seizures and past h/o febrile convulsions (RR=1.93) in the study (Table 6).Positive association was found between symptomatic seizures and past h/o neonatal seizures (RR=1.75) in the study.In the study, positive EEG findings were found in 36 out of 42 cases of idiopathic seizures (85.7%), which mean that there is a strong association between the two (RR= 2.59) (Table 7).



Discussion:
Seizures are a common neurologic disorder in the pediatric age group.It occurs in about 3 – 5% of chil-dren, rates slightly higher in boys. Seizures do not constitute a diagnosis but are primarily a symptom of an underlying central nervous system disorder that requires a detailed history, careful clinical examination and a thorough investigation to arrive at diagnosis and then a judicious management plan.(9)The investiga-tion of a seizure disorder depends on many factors, including age of patient, type of seizure, frequency, presence or absence of neurologic findings and constitutional symptoms.(8)
Distinguishing between epileptic seizures and non-epileptic attack disorder may be impossible even after extensive history taking and detailed investigations. Even migraine may be confused for epilepsy and vice versa. Both migraine and epilepsy may be provoked by exogenous and endogenous factors. Exceptionally a severe migraine may result in an ischemic lesion, which acts as an epileptic focus.(10)
In the study, 42% of cases were diagnosed to have idiopathic seizures. The finding differs numerically from the epidemiologic studies, where in 60 % cases no cause could be attributed by imaging. The gross change in numeric is due to the improvement in imaging techniques and to mention especially MRI, which provides information about subtle abnormalities due to inherent soft-tissue contrast.(11)
There is a strong male preponderance in this study (Male : Female :: 1.7 : 1), which corroborates with study by Eriksson and Koivikko in 1997, reprinted by permission of journal epilepsia, where incidence varies markedly with age and slightly higher ratio seen in case of boys(11).
In the study, etiological diagnosis by neuro-imaging showed:
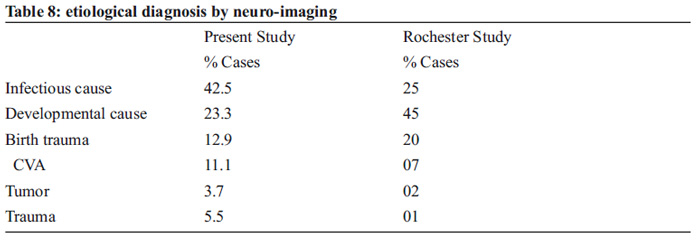
Epidemiological studies in children, which have taken particular care to classify seizure type, have sug-gested that focal epilepsies are more common then generalized epilepsies. In the B.N.C.D. study after 23 years follow up, about 70% of those which seizures were classifiable had focal epilepsies and 30 % had generalized epilepsy, about 45 % of both were symptomatic and probably symptomatic. The type of epi-lepsy could not be determined in around one fifth of subjects. In contrast to this theory, the present study shows Focal Epilepsy in 38.54% cases, and GTC in 48.95% cases. Myoclonic Seizures occurred in 10.4% cases.(12)
Highest incidence of seizures were seen in and around second year of life(1-3 years).Children in the 2nd and 3rd year of life have seizures mostly of infectious etiology. Children in the first year of life present with seizures mainly due to developmental/congenital anomalies or perinatal insults. These children are more prone to myoclonic seizures and usually have past history of neonatal seizures.These children suffer less from infections, partly because of transplacentally transferred maternal antibodies, protection from antibodies in breast milk and immunizations.
In this study, it was found that most seizure cases are of infectious etiology (42.5%) as is expected in a developing country like India. In contrast, developmental or perinatal causes are more common in the West .Infectious etiology is much less there. Perinatal causes have fallen in number in contrast to previous studies because of improved antenatal and perinatal monitoring (13,14).In the study, EEG changes were found in 67 cases, (69.7 % of cases). RR of 2.59 means strong association between positive EEG and childhood seizures.
Prior history of febrile seizures was found in 7 cases of idiopathic seizures, which means approx. 16.6% association between febrile seizures and seizure disorder. RR of 1.93 means a strong association between febrile seizures and subsequent development of idiopathic epilepsy. This corroborates with the communi-ty based study done by Anne T. Berg, Ph.D from the department of Biological Science, and Sholmo shinnar from department of Neurology and Pediatrics, where results showed 13.9% association between prior febrile seizures and childhood seizures. Some studies have shown that febrile seizure precedes epi-lepsy in 10-15 % cases(6).
History of neonatal seizures was present in 25.9% cases of symptomatic childhood seizures. RR of 1.75 means a good degree of association between prior H/O neonatal seizures and symptomatic childhood sei-zures.(13)
Positive neurological signs were seen in 83.3% of symptomatic childhood seizures. RR of 3.4 shows a strong association between abnormal neurological findings and childhood seizures. This means, imaging is recommended for children with seizure disorders who present with abnormal neurological signs.(15) This corroborates with study done by Yang & co-workers as mentioned in review of literature.
Limitations:
The study has some limitations. Firstly, the sample size was small and ictal EEG was not taken in this study. Secondly, the relative risk estimate may increase or decrease as a result of bias that might result in the derivation of statistical assumption.
Conclusion:
In conclusion, we have established that neuro-imaging specially MRI had an incredible role to play in the etiological diagnosis of childhood seizures. There was a strong association between positive neurological signs and symptomatic seizures. Also positive EEG findings aresignificantly associated with idiopathic seizure. Finally, a large prospective study in future is necessary to establish and confirm the results and analysis made in this study.
Author contribution: Dipankar das, Anasua datta -Data collection, Write-up, Swapan kumar ray – Concept, Guidance, Satyaki das -Statistical Analysis
Conflict of Interest: None
Source of Funding: Nil
References:
1. Nordli DR.,Kuroda MM ,Carol J et al; experience with ketogenic diet in infants. Pediatrics 2001;198:129
2. Shinnar S,Pellick JM:Update on the epidemiology & prognosis of childhood of Pediatric Epil ep-sy; J Child Neurol 2002;17:s54:7
3. Mizrahi EM; electroencephalographic / polygraphic / video-monitoring in childhood epilepsy. J Pediatr 1984; 105: 1
4. Gilman S: Imaging the brain Part 1 & 2 N. England J Med 1998; 338; 812
5. Wallace SJ:First tonic clonic seizure in childhood. Lancet 1997;349:1009
6. Berg AT, Testa FM, Levy SR, et al; Neuroimaging in children with newly diagnosed epilepsy: A community based study; Pediatrics 2000; 196:527
7. Otsubo H, Snead C, MRI in children; Journal child neurol. 2000; 16:227-35
8. Camfield CS, Camfield PR Dooly JM, et al: epilepsy after a first unprovoked seizure in child-hood; Neurology 1985; 35:1657
9. Duchowny M Harvey AS: Pediatric Epilepsy Syndromes:an update and critical review. Epilepsia 1996; 37(suppl)US:26
10. Deep ZL,Rothfus WE, Maroon JC: MR Imaging of heterotopic grey matter.J Comput assist to-mography 9:1140,1985
11. Eriksson KJ, Koivikko MJ: Prevalence, classification and severity of epilepsy and epileptic syn-dromes in children. Epilepsia 1997; (Chapter 38; 1275-82)
12. Wong M, Schlagger BL,Landt M;Postictal CSF abnormalities in children.J Pediatr 2001;138:373
13. Volpe JJ; Neonatal Seizures; current concepts & revised classification. Pediatrics 1989,84 : 4 22.
14. Maytal J,Shinnar S;Febrile Status epilepticus , Pediatrics 1990;86:611
15. Zee CS,Segall HD, Miller C,et al: unusual features of intracranial cysticercosis. Radiol 137:397-4071980
Issue: April-June 2018 [Volume 7.2]