Development And Validation Of Trivandrum Development Screening Chart For Children Aged 0-3 Years by TDSC (0-3)
Original Research
Original Research
![]()
Abstract :
Objective: To develop and validate a simple screening tool for identifying developmental delay among children of 0-3years of age in the community.
Methods: The 27-items of Trivandrum Development Screening Chart for children of 0- 3years [TDSC (0-3y)], were carefully prepared from the norms in various existing developmental charts/scales, by experts keeping in mind the face validity. The criterion validity was assessed in a community sample of 400 children of 0-3y with a mean age of 14months (SD of 10.33), including 203(50.75%) boys and 197 (49.25%) girls. TDSC (0-3y) was validated against Denver Developmental Screening Test (DDST) as the ‘Reference Standard’.
Result: When one item delay in TDSC (0-3y) was considered as ‘TDSC delay’ (Test positive), the sensitivity and specificity of TDSC (0-3y) was found to be 86.7% (95% CI: 58.4%-97.7%) and 100% (95%CI 98.8%-100%) respectively with a Negative Predictive Value of 99.5% (95% CI 97.9%-99.9%).
Conclusions: TDSC (0-3y) is a simple, reliable and valid screening tool for use in the community to identify children between 0 and 3 years with developmental delay, enabling early intervention practices.
Keywords: Developmental delay, Screening tool, Validation
Introduction
The term development delay is used when a child’s development lags behind established normal ranges (norms) for his or her age in areas of motor, cognitive, language, behavioral, emotional, or social development delay among children of less than 3years of age is often identified only by professionals, when they are brought for medical advice for other reasons. At the community level, these children are usually not identified due to the lack of a simple tool that can be used by community health worker. Early detection of development delay is important for instituting community based intervention program as possible in an effort to prevent onward progression to disability.
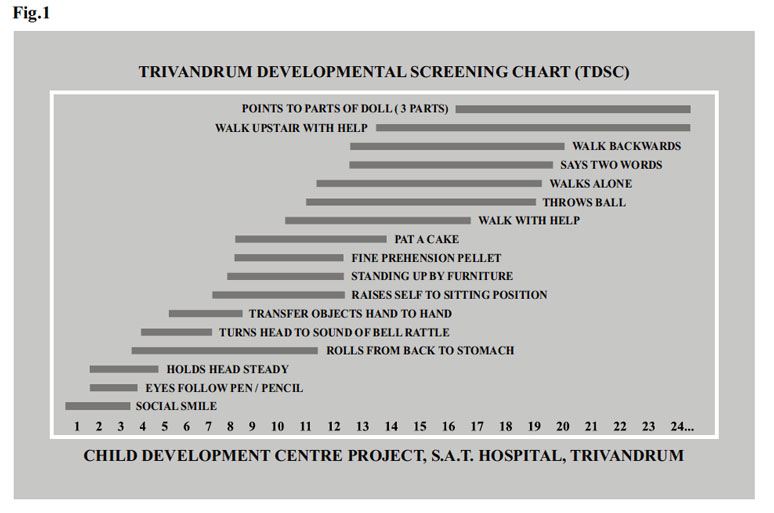
Trivandrum Developmental Screening Chart (TDSC)1 was designed and developed the Child Development Centre, SAT Hospital, Medical College, Trivandrum. Initially seventeen test items were carefully chosen after repeated trial and error method so as to include adequate mental and motor developmental milestones spread over the first 2 years of age. Care was taken to include items for testing hearing and visual functions. There is an over representation of items near one year of age because that is an ideal age for formal developmental assessment in a community setting. The range for each test items was taken from the norms given in Bayley Scales of Infants Development (Baroda norms).2 The left hand side of each horizontal dark line represents age at which 3% of children passed the item and the right end represent the item in the Baroda sample. A vertical line is drawn or a pencil is kept vertical line is drawn or a pencil is kept vertically at the level of the chronological age of the child being tested. It the child fails to achieve any item that falls short on the left side the vertical line, the child is considered to have developmental delay. Any obvious abnormality or asymmetry is also considered abnormal. The term development delay is used when a child’s development lags behind established normal ranges (Norms) for his or her age in areas of motor, cognitive, language, behavioral, emotional, or social development delay among children of less than 3 years of age is often identified only by professionals, when they are brought for medical advice for other reasons. At the community level these children are usually not identified due to the lack of a simple tool that can be used by community health worker. Early detection of development delay is important for instituting community based intervention program as possible in an effort to prevent onward progression to disability.
Trivandrum Developmental Screening Chart (TDSC) (Fig.1) was designed and developed at the Child Development Centre, SAT Hospital, Medical College, and Trivandrum. Initially seventeen test items were carefully chosen after repeated trial and error method so as to include adequate mental and motor developmental milestones, spread over the first 2years of age. Care was taken to include items for testing hearing and visual functions. There is an over representation of items near one year of age because that is an ideal age for formal developmental assessment in a community setting. The range for each test items was taken from the norms given in Bayley Scales of Infants Development (Baroda norms).2 The left hand side of chart each horizontal dark line represents age at which 3% of children passed the item; and the right end represent the item in the Baroda sample. A vertical line is drawn or a pencil is kept vertically on the chart at the level of the chronological age of the child being tested. It the child fails to achieve any item that falls short on the left side the vertical line, the child is considered to have developmental delay. Any obvious abnormality or asymmetry is also considered abnormal. The Denver Development screening Test (DDST) (Fig.2) is commonly known as the Denver Scale. It was developed by William K. Frankenburg and first introduced by him and Josiah. B. Dobbs in 1967. The test cover four functions: gross motor, language, fine motor-adaptive, and personal-social.
Nair and et al also had done a similar study – Development and Validation of Trivandrum Development Screening Chart for children Age 0- 6years [TDSC (0-6)] 4. In their study, 51-items of Trivandrum Development Screening Chart for children of 0-6 y [TDSC (0-6y)] were included. In our current study 27-items of Trivandrum Development Screening Chart for children of 0-3 y [TDSC (0-3y)] (Fig. 1), were included. Nair and et al study validity was assessed in a community sample of 1,183 children of 0-6 y with a mean age of 35.38 months (SD of 19.25) including 597 (50.46%) boy and 586 (49.54%) girls.
In our study, the validity was assessed in well baby clinic sample of 400 children of 0-3 years, with a mean age of 14 months (SD of 10.33), including 203(50.75%) and 197(49.25%) girls.
Nair and et al study TDSC (0-6y) was validated against Denver Developmental Screening Test (DDST) as the ‘Reference Standard’ (Fig. 2). In our study TDSC (0-3y) was also validated against DDST as the ‘Reference Standard’. Nair and et al study one item delay in TDSC(0-6y) was considered as ‘TDSC delay’ (Test positive), the sensitivity and specificity of TDSC (0-6y) was found to be 84.62% (95%CI 71.92-93) and 90.8% (95%CI 88.97-92.43) with a Negative Predictive Value of 99.23% (95% CI 98.48-99.67). In our study one item delay in TDSC (0-3Y) was considered as ‘TDSC delay’ (Test positive), the sensitivity and specificity of TDSC (0-3Y) was found to be 86.7% (95% CI: 58.4%-97.7%) and 100% (95%CI98.8%-100%) respectively with a Negative Predictive Value of 99.5% (95% CI 97.9%-99.9%).
Methodology
Aim: Identifying developmental delay among children of 0-3years of age in the community.
Objective: To develop and validate a simple screening tool for identifying developmental delay among children of 0-3yr of age in the community.
Study type: This is a cross section study.
400 children between 0 -3 years, from Well Baby Clinic of M.G.I.M.S. Kasturba Hospital, Sewagram, Wardha. Sample included all children with proper consent and willingness to participate in the study. Exclusion included those who were ill and non-testable.
Tool: Trivandrum Developmental Screening Chart for children of 0-3 years was designed and developed at the Child Development Centre, SAT Hospital, Medical College, Trivandrum. Tool items (27 in number were carefully chosen, from the item pool, after repeated discussions with experts (Pediatrics Neurologists, Child Psychiatrists, Clinical Psychologists, Developmental Pediatrics, Developmental Therapists, Speech therapists and Epidemiologists) to include adequate cognitive and motor milestones, which are adequately spread over the first 3 years of life. Care was taken to include a few items for testing hearing, vision, speech and language also. Where ever possible, the item selection was done from tools where normative validation was available.
For the new tool to apply, the chronological age of the child is obtained first. Then a line is to be drawn vertically through the chronological age of the child (Given in the bottom horizontally) marked in the tool. The items with upper limit ending to the left of the line are expected to be attained by the child normally. If any item is not attained by the child by that age, that item delay is assumed for the child. Thus, the tool is designed to be simple and no expertise is required, when compared with DDST. For the new tool prematurity corrections are not done for calculating the chronological age of the child, as this would make the tool complicated and the authors feared that such corrections would make it unsuitable for persons like an Angnwadi worker to use it in the community, although such corrections (For preterm babies) are bound to improve positive predictive value and specificity.
Validation of TDSC (0-3Y)
The total sample for validation was calculated as follows. N (Number of positives for developmental delay) was calculated using the formula N=(1.96)2PQ/d2, where P is the sensitivity expected, Q is (1-P) and d is the precision desired. Keeping the expected sensitivity of the new tool as 90% (After pilot study) and precision 10% and with 95% confidence interval, the sample calculated was 15 positive cases (Of developmental delay). Assuming 1% prevalence for developmental delay in 0-3 y age group, the total sample required was calculated as 400. Sample included all children, with proper consent and willingness to participate in the study. TDSC (0-3Y) was validated against Denver Developmental Screening Test (DDST) as the ‘Reference Standard’.The Denver Development screening Test cover four functions: gross motor, language, fine motor-adaptive, and personal-social.
400children from birth to 3 years old, were taken from Well Baby Clinic of M.G.I.M.S. Kasturba Hospital, Sewagram, and Wardha. Sample included all children with proper consent and willingness to participate in the study. Exclusion included those who were ill and nontestable. The screening test and the ‘Reference Standard’ were administered by independent observers blinded to the results of the other tests. The first child received TDSC first and DDST next while the seconds child received the DDST first and TDSC next and so on; till the study was completed. Administration procedures for the tests were standardized. TDSC (0-3y) was applied by the author herself, after getting written consent from the parents and verbal assent from the child, whenever possible. Data was analyzed using statistical functions available in Microsoft exel and Epi 6.04 statistical software. Criterion validity depends on the criterion measurement and ideally, the criterion should reflect the ‘Absolute truth’, and is commonly referred to as the ‘Gold standard’/ ‘Reference standard’. Sensitivity, Specificity, Positive Predictive Value, Negative Predictive Value and Likelihood Ratios (Positive and negative) for TDSC (0-3Y) against DDST as ‘Reference Standard’ were calculated.
Results
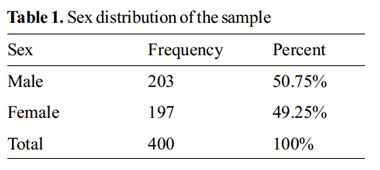
A total of 400 children were selected for validation including 203 (50.75%) boys and 197 (49.25%) girls.

Year wise distribution of the sample (Table 2) shows that maximum number of sample from age group 7- 12monthswere153(38.25%) and minimum number sample from age group of 25-30months were 3(10.75%).
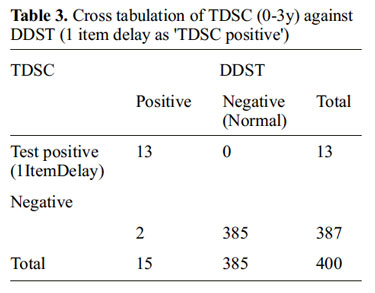
Cross tabulation of TDSC having one item delay as test criteria positive (‘TDSC delay’) against DDST positive are given in table 3 above. There were 13 true positives and 385 true negative out of 400 children, who had total assessment. DDST categorized ‘Abnormal’ as Reference standard positive. All others were negative.
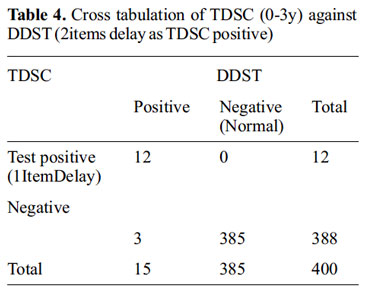
The cross tabulation of TDSC with two items delay as test criteria positive (‘TDSC delay’) against DDST positive are given in the table 4. There were 12 true positives and 385 true out of 400 children, who had total assessment.
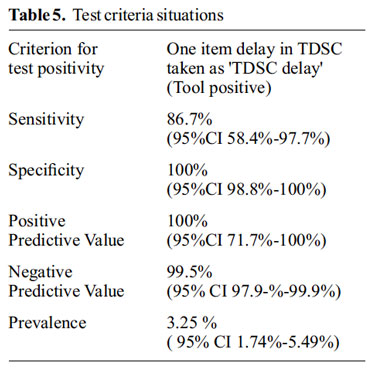
Table 5 shows the comparison of test characteristics in two situations of the test (tool) criteria-having one item delay as ‘TDSC delay’.

Table 6 shows the comparison of test characteristics in two situations of the test (Tool) criteria, having two items delay as ‘TDSC delay’.
As an alternate strategy we also explored other methods in calculations like calculating Kappa of the sample with DDST. Here the DDST result was interpreted as positive when the child is categorized as either abnormal or questionable and all others as ‘normal’. This calculation gives a ‘Second’ reference standard from the same test result of DDST.
Discussion
A developmental screening tool for community screening should be simple, less time consuming, easily understood by the community health worker, parents and should cover all developmetal domains. TDSC (0-3Y) meets all these criteria. According to a study commissioned by the Public Health Agency of Canada, DDST is the most widely used test for screening developmental problems in children.8 However DDST and DDST-II 9, required more expertise and hence not considered suitable as a screening tool for a community health worker. The author feels that TDSC (0-3Y) is a simple, convenient and valid Indian tool, for idendtifying children of 0-3years with developmental delay in the community.
In this study, the ‘TDSC delay’ (Tool positivity) sensitivity was found to be 86.7% with specificity 100%. TDSC was developed as a screening tool for developmental delay; as test positive accepting a specificity of 99.48%. In this situation, one item delay as test positive gives an excellent ‘Negative Predictive Value’ of 99.5%, which is desirable for a screening tool. A screening test should ideally be one with a high Sensitivity, high Negative Predictive Value and not having much compromise on Specificity. TDSC satisfies these criteria.
Positive Predictive Value obtained for this selection (One item delay) was expected in a situation where the specificity was relatively good (100%). This Positive Predictive Value is explained and justified by the relatively large number and the low prevalence (3.25%) of developmental delay in the sample studied (Though the prevalence is ‘significant’ to the community).
We selected original DDST itself (among the two) as ‘reference standard’ though imperfect because of relatively higher specificity of original DDST compared with DDST-II.10-12 Thus the original DDST is a better reference/gold standard test than DDSTII (Which is more inclined towards a screening tool/test) to assess their new tool. In absence of a ‘perfect reference standard’ a researcher, as a compromise, will be reference standard and in these situations the kappa statistics is commonly used to assess agreement for estimating the “validity”. As an alternate strategy, we also explored other methods like calculating Kappa of the sample with DDST and found that there is an excellent agreement.
Summary and conclusion:
The 27-items of Trivandrum Development Screening Chart for children of 0-3years [TDSC (0- 3y)], were carefully prepared from the norms in various existing developmental charts/scales by experts, keeping mind the face validity. The criterion validity was assessed in a community sample of 400 children of 0-3years age with a mean age of 14months (SD of 10.33) including 203(50.75%) boys and 197 (49.25%) girls. TDSC (0-3Y) was validated against Denver Developmental Screening Test (DDST) as the ‘Reference Standard’.
When one item delay in TDSC (0-3Y) was considered as ‘TDSC delay’ (Test positive). The sensitivity and specificity of TDSC (0-3y) was found to be 86.7% (95% CI: 58.4-97.7%) and 100% (95%CI98.8%-100%) respectively with a Negative Predictive Value of 99.5% (95% CI 97.9%-99.9%).
Conclusion:
TDSC (0-3Y) is a simple, convenient and valid screening tool for identifying children of 0- 3years age with developmental delay in the community. This is a tool, which can be accomplished in 10minutes by a health worker. It requires, apart from the tool, a pen/pencil and some preliminary training to apply the tool. This helps in community intervention programs and if needed, refer the child at the earliest for appropriate intervention to a nearby referral centre. This tool is not for assessing the developmental age of the child and for a specific diagnosis of a developmental delay/disability.
C VH-Reviewed literature and did analysis and discussion, VKY- concept and design of study, KM- carried out clinical work
References:
1. Nair MKC, George B, Philip E, MA Lekshmi MA, Haran JC, Sathy N. Trivandrum developmental screening chart. Indian Pediatr. 1991; 28:869-7.
2. Phatak P. Mental and Motor Growth of Indian Babies(1month-30months). Final report, Development of Child Development, MSUB, Baroda,1973.
3. Frankenourg WK, Dobbs JB. The Denver developmental screening test. J Pediatr. 1967; 71:181-91.
4. Nair MKC, Nair Harikumaran, George B, Suma N, Neethu, Leena M.L, Paul Swamidhas Sudhakar Russell. Development and Validation of Trivandrum Development Screening Chart for children Age 0-6years [TDSC (0-6)], Indian J Pediatric, Special supplement on adolescent care counseling. Published online:08 September 2013.
5. Nair MKC, Radhakrishnan SR, Early childhood development in deprived urban settlements. Indian Pediatr.2004;41:227-37.
6. Kaur P, Chavan BS, Lata S, Kaur A, Tinku S, Arora Y, et al. Early intervention in developmental delay, Indian J Pediatric 2006;73:405-8.
7. Mathur GP, Mathur S, Singh YD, Kushwaha KP, lile SN. Detection and prevention of childhood disability with the help of Anganwadi workers. Indian Pediatr.1995;32;773-7
8. Canadian task Force on the Periodic Health Examination. The Canadian Guide to Clinical Preventive Health Care.Chapter 26 “Preschool Screening for Developmental Problems”. Ottawa: Minister of Supply and Services Canada; 1994.
9. Frankenburg WK, Dodds J, Archer P, Shapiro H, Bresnick B. The Denver II: A major revision and restandardization of the Denver developmental screening test.Pediatrics.1992;89:91-7
10. Greer S, Bauchner H, Zuckerman B. The Denver developmental screening test: How good is its predictive validity? Dev Med Child Neurol. 1989;31:774–81.
11. Glascoe FP, Byrne KE, Ashford LG, Johnson KL, Chang B Strickland B. Accuracy of the Denver-II in developmental screening.Pediatrics. 1992;89:1221–5.
12. Borowitz KC, Glascoe FP. Sensitivity of the Denver developmental screening test in speech and language screening. Pediatrics.1986;78:107
Issue: July-September 2016 [Volume 5.3]