Abstract:
We studied knowledge, attitude and practices prevalent among practicing pediatricians. Focus was on issues in Pediatric Gastroenterology & Hepatology. Multiple Choice Question based format was given to Pediatricians and their response was noted and analyzed. Interesting observations were discussed and analyzed.
Keywords- Paediatric gastroenterology and hepatology, Recurrent vomiting,Upper GI Haemorrhage, TORCH, Neonatal Cholestasis, Hepatitis
Introduction:
Pediatric Gastroenterology is one of the developing pediatric subspecialties in India. Spectrum of issues includes GI luminal conditions, Hepatology, Pancreatic diseases, and Nutritional disorders. Numbers of Pediatric Gastroenterologists practicing in India are few as compared to Pediatricians. Pediatric gastroenterology as a branch faces many different challenges in current scenario. Many of the disorders cared in Pediatric Gastroenterology are chronic and have short & long term impact. Management strategies for these conditions need to encompass team approach, with an emphasis upon optimal care. This study reinforces the need to study prevalent practices and management styles, subsequently direct the resources for early identification and proper treatment of kids with GI and liver diseases.
Material and Method:
The study was done after consent from practicing pediatrician between March 2016 to November 2016.Those who refused consent were not enrolled. Pediatricians were assured regarding nondisclosure of identity & confidentiality. 216 pediatricians from states of Central India viz Maharashtra, Madhya Pradesh & Chhattisgarh who were qualified MD /DNB/DCH were enrolled.KAP (knowledge, Attitude, Practices) were analyzed and studied. Pediatricians were given questionnaire, 12 questions in MCQ (Multiple choice questions) format. Topics included in questionnaire viz. recurrent vomiting, upper Gastrointestinal(GI) bleed, neonatal cholestasis(NCS), probiotics, acute gastroenteritis, hepatitis & liver failure, pancreatic issues, pediatric endoscopy and constipation in children. The rare diseases like metabolic liver disease were not included in the study. The chief objective being to analyze common disease management practices. The questionnaire was prepared to involve all common issues faced by child care professional in pediatric gastroenterology &hepatology. The data collected was analyzed.
Analysis:
Issue 1: Recurrent vomiting in children:
Many children were seen in busy practice for off and on vomiting. Symptomatic management is commonly done with treatment of underlying cause. Kids with recurrent vomiting are frequently missed and inappropriately managed.
In this question 4 options were given. About 61% pediatricians felt that those kids who have recurrent vomiting and failure to thrive need further investigations. While 27% of pediatricians feel nocturnal vomiting was a red flag sign. 8% of pediatricians feel need to further investigate cases that have associated dysphagia. About 97% were not comfortable to investigate happy spitters in infancy.
{kind=link}
Upper gastrointestinal bleeding can be variceal or non-variceal. First contacts of these kids are pediatricians managing at peripheral centers. Blood transfusion pattern or strategies are varying from place to place. We included this question to study the Practices followed.
About 41% of pediatricians felt hemoglobin (Hb) to be 10 gm/dl while 32% felt safer hemoglobin levels are 7 gm/dl to avoid re-bleed in cases of portal hypertension. 20% of child care professionals would like to keep Hb of 8 gm/dl while approximately 6% felt the need to raise the hemoglobin to 12 gm/dl.
{kind=link}
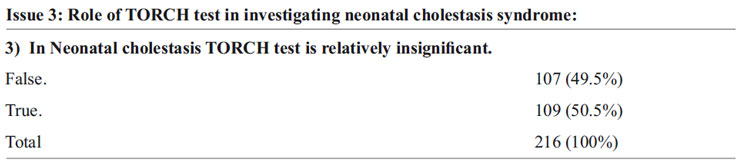
TORCH test (Toxoplasma, Rubella, Cytomegalovirus, Herpes, others) is the commonly asked test by pediatrician. Frequently ordered but rarely used to change the management of neonates with direct hyperbilirubinemia .House was equally divided on this issue. About 50% of pediatricians felt TORCH test is not contributing to their management of patients with neonatal cholestasis.
{kind=link}
This issue was placed in true/false format. New born jaundice with yellow urine and clay color stool is a clinical marker for neonatal cholestasis .The frequent late referral and inappropriate diagnosis make management of neonatal cholestasis patients’ difficult. Biliary atresia and metabolic disorders are often missed. Our survey underscored that 85% of pediatricians agreed to investigate any newborn with jaundice with/without pale stool and yellow urine for neonatal cholestasis.
{kind=link}
Oral rehydration is the corner stone in management of acute gastroenteritis in children .Probiotics are increasingly used in practice. Many preparations are available in market. Few are studied. Evidence base is available with fewer .About 93%pediatricians would prefer saccharomyces boulardii while 31% prefer lactobacillus GG. Bacillus clausii preference as probiotics for acute gastroenteritis among pediatrician was 3%.
{kind=link}
38% pediatricians felt that INR (international normalized ratio) was an important factor to differentiate between hepatitis and acute liver failure. 26% felt the need for clinical signs of encephalopathy to be present to define liver failure .12% gave importance to elevated liver enzymes and 24% required raised ammonia to categorize liver failure.
{kind=link}
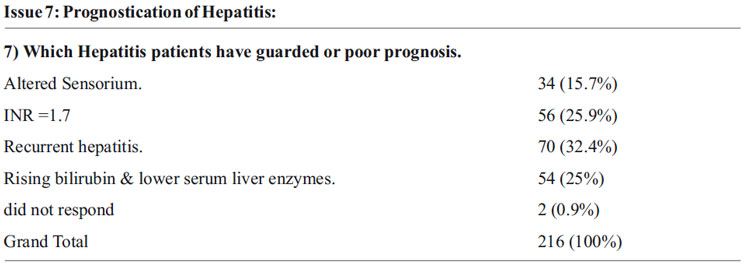
16% of pediatricians felt altered sensorium in a hepatitis patient to have poor prognosis. 26% gave importance to deranged INR which was suggestive of coagulopathy. Rising bilirubin and lowering liver enzymes was considered as poor prognostic factor by 25% of pediatricians.2 pediatricians did not answer the question.
{kind=link}
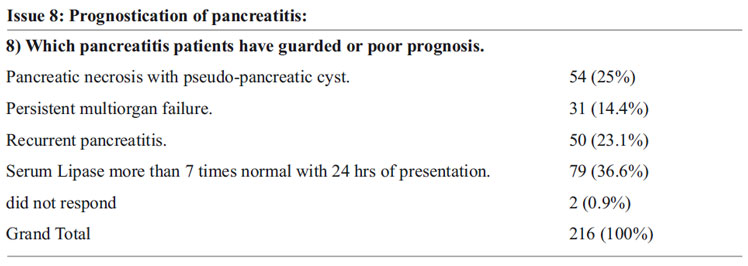
Acute pancreatitis is commonly managed by Pediatricians. Sr. Lipase more than 7 times normal within 24 hours of presentation was considered to have a poor prognosis by approx. 37% of pediatricians. 25% felt pseudo-cyst of pancreas and necrosis to be a bad prognostic indicator. Multi organ failure and recurrent pancreatitis was considered correlating with poor generalized outcome by 14% and 23% health care professional respectively.
{kind=link}
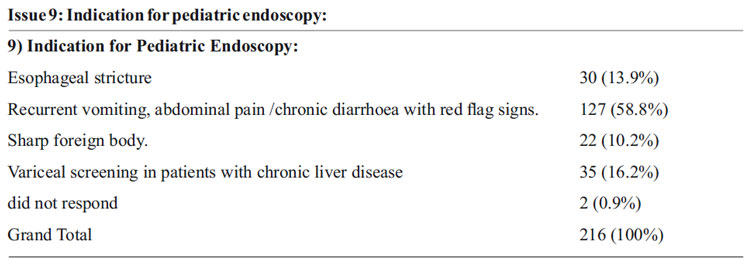
Very few pediatricians are exposed to pediatric endoscopy in India in their post graduate curriculum. Among pediatricians 58% agreed to endoscopy a child with recurrent vomiting, abdominal pain or chronic diarrhea with red flag sign on history taking and clinical examination. Only 14% were comfortable to diagnose and do endoscopy for esophageal stricture. 16% were agreeing for endoscopy with chronic liver disease for variceal screening while only 10% had given affirmation to do endoscopy for sharp foreign body removal.2 pediatrician did not exercise their right to answer this question.
{kind=link}
Pediatric constipation is an important cause of referral to Pediatric gastroenterologist. Appropriate diagnosis and management of these patients is the need of hour.
In our Survey 3% felt need for behavioral modification for treatment of constipation .30% stressed to diet modification. 48% of health care professionals agreed to go ahead with rectal dis-impaction followed by maintenance therapy. 20% felt duration of laxative therapy to be sufficient if treated for 7-10days.
{kind=link}
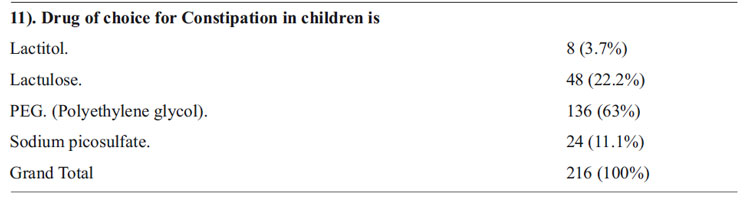
63% of pediatricians felt drug of choice for constipation in children is PEG
(Polyethylene glycol).About 23% relied on lactulose. 11% preferred sodium picosulfate.
{kind=link}
23% felt duration of therapy for constipation was 1 week. 26% agreed for 2 to 3 weeks of treatment. 40% were willing to use therapy for 2 months .10% extended duration for more than 2 months.
Discussion:
KAP studies are used to assess knowledge, attitude and styles of practice. There are papers on such studies on Helicobacter pylori infection 1 Gastro-esopahgeal reflux disease2 published. Our study focuses on more than one issue or disease. It is broad based. Multiple variables were considered.Common symptomatic approach, basic clinical tools, preferences of pediatricians for investigations & drug used were studied in MCQ format.
Pediatricians were clearly well informed on most of the issues. Importance of growth charts in OPD practice is reinforced when most participants agreed to investigate further on kids with recurrent vomiting and failure to thrive. The most common time of onset for cyclical vomiting syndrome is at night (3) In our study many pediatricians considered this as a red flag sign.
The hemoglobin threshold for transfusion of red blood cells in patients with portal hypertension is studied earlier in many studies. Some favor liberal transfusion while some are proponent of restrictive pattern. Restrictive strategy significantly improved the outcome in patients with upper GI bleed 4. Multiple mechanisms were proposed to avoid over transfusion in these cases e.g. clot rupture, coagulopathy, immunomodulation 4 Hemoglobin of 8 gm/dl is recommended in guidelines on prevention and management of gastro-esophageal varices and variceal hemorrhage in cirrhosis in Baveno IV criteria to avoid increase in portal pressure. 5, 15 The target hemoglobin should be between 7-8 gm/dl 6
Limitation of TORCH test is increasingly known to have low diagnostic yield. 7 Still 50% of pediatrician does feel doing TORCH TEST and that would change to management in neonatal cholestasis.
Management guidelines on neonatal cholestasis are well studied now in Indian scenario 8 Increased sensitivity among pediatricians to pick neonatal cholestasis cases is noted in our study which is definitely encouraging news for Indian Academy of Pediatrics (IAP) & Indian Society of Pediatric Gastroenterology, Hepatology & Nutrition (ISPGHAN)
Lactobacillus rhamnosus GG and saccharomyces boulardii are considered in management of AGE in children 9,10,16.
Liver function tests are important tool for health care professional to assess liver biochemically. It is important to note that normal ALT may not exclude significant liver disease. Pediatric Acute Liver failure is defined as evidence of liver dysfunction within 8 weeks of onset of symptoms and uncorrectable coagulopathy with international normalized ratio INR >= 1.5 in patients with hepatic encephalopathy or INR > 2.0 without encephalopathy and no evidence of chronicity11 underscores INR as important tool to distinguish hepatitis and liver failure. Relatively low i.e. 38% felt importance of INR while 26% gave importance to signs of encephalopathy in our study.
Sr. Lipase level higher than 7 times normal within 24 hours of onset of disease predicts poor prognosis. 12 In our study 37% gave weight-age to this biochemical finding. The complications of pancreatitis were well judged by practicing pediatrician.
Weight loss, failure to thrive are important diagnostic indication for doing pediatric endoscopy in cases of chronic diarrhea, recurrent vomiting. 14 Correlation of Gastrointestinal luminal symptoms with failure to thrive are rightly judged by most of pediatricians. Awareness about GI luminal management of pediatric stricture is poor as per our survey. Reviewed literature suggest that endoscopy can be considered with underlying chronic liver disease with increasing liver stiffness and Low platelet count 6 Our study highlights the need for sensitization and continued medical education in this area of pediatric endoscopies. Only 10% were willing for endoscopic sharp foreign body retrieval.
Polyethylene glycol (PEG) is more effective than lactulose ,milk of magnesium or mineral oil for management of pediatric constipation 13 Based on expert opinion in guideline maintenance therapy following dis-impaction is recommended to continue for at least 2 month 13 In our study various duration treatment protocols were used by pediatricians.
Conclusion:
The main aim of study is not to judge any health care professional but to understand prevalent practices. Our KAP study includes Pediatric Gastroenterology and Hepatology diseases commonly seen by pediatricians. We focused on multiple issues and variables. Deviation from literature and guideline was noted in some areas. Needs to en-strengthen academic activities in those fields is reinforced by our study.
Main limitation of our study is small sample size .Structured MCQ format without any scope for clinical discussion with participating pediatrician jeopardizes the choice attended by him / her. But this is one of its own kind KAP study. In current era the awareness of pediatric gastroenterological issues in practice, knowledge about recent advances and practices prevalent are necessary to be understood to develop further academic program by Pediatric and Pediatric Gastroenterology societies. The team work between pediatricians & pediatric gastroenterologist is necessary. Follow up KAP studies are needed to be planned in future for post implementation assessment of directed academic programs.
References:
1. Diaz, Diego M; Winter, Harland S Colletti,et al Knowledge, Attitudes and Practice Styles of North American Pediatricians Regarding Gastroesophageal Reflux Disease Journal of Pediatric Gastroenterology & Nutrition: July 2007 – Volume 45 – Issue 1 – p 56-64
2. Chang, Howard Y.*; Sharma, Virender K,et al. Knowledge, Attitudes, and Practice Styles of North American Pediatric Gastroenterologists: Helicobacter pylori Infection Journal of Pediatric Gastroenterology & Nutrition: February 2003 – Volume 36 – Issue 2 – pp 235-240
3. Li BUK, Fleisher DR. Cyclic vomiting syndrome: features to be explained by a pathophysiologic model. Dig Dis Sci. 1999;44:13S-18S
4. Hebert PC, Timmouth A, Corarin HL. Contraversies in RBC transfusion in critically ill chest 2007 may 13 (5) 1583-90
5. De Franchis, Roberto Evolving Consensus in Portal Hypertension Report of the Baveno IV Consensus Workshop on methodology of diagnosis and therapy in portal hypertension Journal of Hepatology , Volume 43 , Issue 1 , 167 – 176
6. De Franchis, Roberto Expanding consensus in portal hypertension Journal of Hepatology , Volume 63 , Issue 3 , 743 – 752
7. Shet A Congenital and perinatal infections: throwing new light with an old TORCH Indian J Pediatr. 2011 Jan;78(1):88-95. doi: 10.1007/s12098-010-0254-3. Epub 2010 Oct 16
8. Bhatia V, Bavdekar A, Matthai J, Waikar Y, Sibal A. Management of neonatal cholestasis: consensus statement of the Pediatric Gastroenterology Chapter of Indian Academy of Pediatrics. Indian Pediatr. 2014 Mar;51 (3): 203-10.
9. SzajewskaH1,GuarinoA, HojsakI,etalUseof probiotics for management of acute gastroenteritis: a position paper by the ESPGHAN Working Group for Probiotics and Prebiotics. J Pediatr Gastroenterol Nutr. 2014 Apr;58(4):531-9.
10. Guarino A1, Ashkenazi S, Gendrel D, etal European Society for Pediatric Gastroenterology, Hepatology, and Nutrition/European Society for Pediatric Infectious Diseases evidence-based guidelines for the management of acutegastro-enteritis in children in Europe: update 2014. J Pediatr Gastroenterol Nutr. 2014 Jul;59(1): 132-52
11. Pediatric Gastroenterology Chapter of Indian Academy of Pediatrics1, Bhatia V, Bavdekar A, Yachha SK; Management of acute liver failure in infants and children: consensus statement of the pediatric gastroenterology chapter, Indian academy of pediatrics. Indian Pediatr. 2013 May 8;50(5):477-82.
12. Banks PA, Freeman ML; Practice guidelines in acute pancreatitis.Am J Gastroenterol. 2006 Oct;101(10):2379-400.
13. TabbersMM, DiLorenzoC, BergerMY, etalEvaluation and treatment of functional constipation in infants and children: evidence-based recommendations from ESPGHAN and NASPGHANJ Pediatr Gastroenterol Nutr. 2014 Feb;58(2):258-74.
14. Andrea Tringali, Mike Thomson2, Jean-Marc Dumonceau3, et al Pediatric gastrointestinal endoscopy: European Society of Gastrointestinal Endoscopy (ESGE) and European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) Guideline Executive summary Endoscopy 2017; 49(01): 83-91
15. Waikar. Y. Portal hypertension. Recent advances in pediatrics 23 pediatric gastroenterology, hepatology and Nutrition (15) : 211 – 222.
17. Waikar. Y. Probiotics, recent advances in pediatric-23, pediatric gastroenterology hepatology and nutrition (15) 404 – 410.
Issue: October-December 2017 [Volume 6.4]