Abstract:
Introduction- Neonatal seizures indicate significant neurological dysfunction or damage to the immature nervous system. It is essential to determine the etiology of seizure at the earliest because it gives an opportunity to treat the seizure actively and promptly and avoid preventable morbidity, mortality and sequelae associated with it. This study was undertaken to study the clinical features, etiology, biochemical abnormalities in neonates with seizures and correlate the biochemical abnormalities with clinical features and etiology of neonatal seizures. Methodology- In this prospective observational study a total of 250 newborns admitted to NICU less than or equal to 28 days of age, with clinically identified seizures were included. A detailed maternal history, complete clinical examination, anthropometry, investigations and treatment given to neonates were noted down and statistical analysis was performed. Results- Incidence of neonatal seizures was 3.70%. Neonatal seizures were more common in first 72 hours (3 days) of life. Subtle seizures were the most common type of neonatal seizures. Neonatal seizures were found to be seven times more common in preterm infants than in term infants. Hypoxic ischemic encephalopathy was the most common cause of neonatal seizures seen in 34.4%.cases followed by Infection. Conclusion- Higher incidence of neonatal seizures was seen in preterm babies (14.35%), low birth weight babies (8.19%) and male neonates. Neonatal seizures were most common in first three days of life. Primary biochemical abnormalities without other comorbid states which could account for the seizures were seen in 20.4 % cases, hypoglycemia and hypocalcaemia were the commonest in this group. Hypoxic ischemic encephalopathy was the most common cause of neonatal seizures seen in 34.4% cases followed by Infection. 25.2% of cases of neonatal seizures with identifiable etiology had biochemical abnormality.
Key Words: Neonatal Seizures, Hypoxic ischemic encephalopathy, Hypoglycemia, Hypocalcaemia, Subtle seizures.
Introduction:
Seizures during the neonatal period are relatively common, occurring in approximately 1.8 to 3.5 per 1000 live births, with greater frequency in premature or low birth weight babies as compared to term babies 1. Neonatal seizures indicate significant neurological dysfunction or damage to the immature nervous system2. The highest incidence of neonatal seizures occurs during the first 48 hours of life3.
Neonates may exhibit some neuroprotection from prolonged seizures, but brief, recurrent seizures can result in significant, permanent changes in the central nervous system, an increased risk of epilepsy, and long term cognitive disabilities4. It is essential to determine the etiology of seizure at the earliest because it gives an opportunity to treat the seizure actively and promptly and avoid preventable morbidity, mortality and sequelae associated with it5.
The neonate is at particular risk for development of seizures because of metabolic, anoxic, structural and infectious causes, although no causes can be identified in one fourth cases6.
This study was undertaken to study the clinical features, etiology, biochemical abnormalities in neonates with seizures and correlate the biochemical abnormalities with clinical features and etiology of neonatal seizures.
Methodology:
This study was conducted in a tertiary care rural hospital in central India. In this prospective observational study a total of 250 newborns admitted to NICU less than or equal to 28 days of age, with clinically identified seizures were included after IEC approval and informed consent from parents. A detailed maternal history, neonatal history with regard to gestational age, perinatal asphyxia, traumatic delivery, septicemia, meningitis, intracranial bleed and hyperbilirubinemia was taken along with detailed history about age of occurrence of first seizure, duration of seizure, number of seizures, type of seizure, course of seizures. Complete clinical examination, anthropometry, investigations and treatment given to neonates were noted down. All the cases were subjected to following investigations- Complete blood count, Blood Glucose, Serum calcium, Serum magnesium, Serum phosphorus, Serum sodium, Serum potassium, Serum chloride. Cerebro-Spinal fluid examination, Blood culture Sensitivity, EEG, Neurosonography & Neuroimaging was done when indicated. Seizures were classified according to classification given by Hill and Volpe in 1994 7 as Primary Metabolic Seizures and Non Metabolic Seizures. Statistical analysis was performed using the statistics software SPSS for windows (17.0 SPSS, Chicago). The analysis of Student’s t-test was used for comparisons of means. Categorical variables were compared using Chi square test and Fischer’s exact test.
Observations And Results:
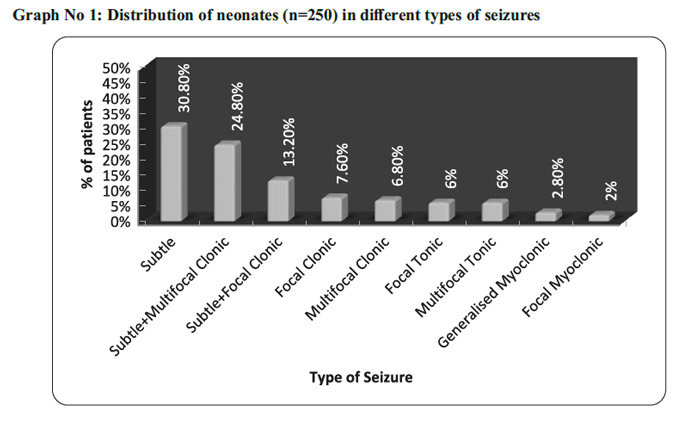
Out of 6752 babies born during the study period, 250 developed neonatal seizures, the overall incidence was 3.70%. Incidence of neonatal seizures in the inborn babies was 2.72% and that of outborn babies was 12.53%.The incidence was high in the outborn babies as compared to inborn babies which is statistically significant. In this study neonatal seizures were more common in preterm and low birth weight neonates. Neonatal seizures were more common in first 72 hours (3 days) of life (Table No 1). Subtle seizures were the most common type of seizures (Graph No 1). . Out of total 250 cases, majority of cases that is 97 (38.8%) cases had seizures due to hypoxic ischaemic encephalopathy (HIE) followed by Infection found in 73 (29.2%) cases (meningitis and sepsis), Metabolic in 51(20.4%) cases, IC bleed in 21 (8.4%) cases, Kernicterus and Congenital malformation of brain (Developmental defect ) in 4(1.6%) cases each (Graph No 2)
{kind=link}
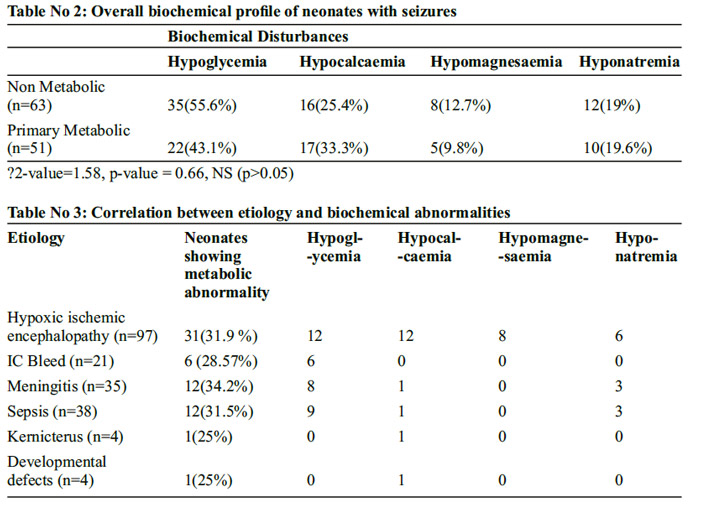
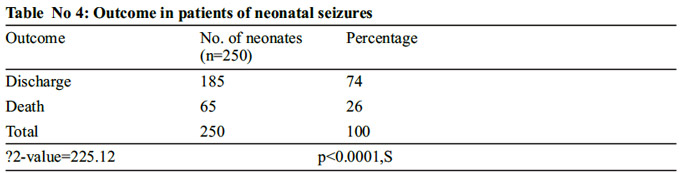
In both primary metabolic and in non metabolic neonatal seizures groups hypoglycemia followed by hypocalcaemia were the major biochemical disturbances found. (Table No 2). Associated biochemical abnormality was found maximum in meningitis followed by Hypoxic ischemic encephalopathy (Table No 3). Subtle seizures were the most common seizures in hypocalcaemia and hypomagnesaemia while multifocal clonic seizures were the most common type in hypoglycemia and hyponatremia (Graph No 3). One fourth patients with neonatal seizures died, where as three fourth patients were salvaged (Table No 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion:
In our study the overall incidence of neonatal seizures was 3.70%, in a study by Bagla et al 8 the overall incidence of neonatal seizure was 11.93 per 1000 live births, the National Neonatal-Perinatal Database (NNPD)9 of India that collated information from 18 centers across the country in the year 2002-03 had reported an incidence of 1.0%. If compared with the majority of studies the incidence of Neonatal seizures was high in our set up and this could be attributed to the tertiary care status of our Institute where high risk and seriously ill newborns are referred for further management.
An overall male to female ratio was 1.27:1 in this study with male preponderance which is consistent with other studies. Cockburn et al10, Fredrichsen11 and Intyrel MC12 also reported male sex preponderance in their studies for which no plausible mechanism has been proposed. In Indian set up this male preponderance could be due to social beliefs; male children may be cared for better than the females.
In this study neonatal seizures were more common in preterm and low birth weight neonates. In our study the incidence of neonatal seizures in preterm babies was 14.3% in contrast to term babies which was 2.03%. Neonatal seizures were found to be seven times more often in preterm infants than in term infants. Gabriel M. Ronen et al13 in a study found that neonatal seizures occur six times more often in preterm infants than in term infants. Kumar et al14 in his study found significant difference in the incidence of term (0.69%) and preterm (6.14%) neonates with seizures in which preterm incidence was far more than term incidence.
Overall incidence of neonatal seizures in low birth weight babies was 63.2 % and 36.8% in normal weight newborns. Holden KR et al 15 found that the incidence of neonatal seizure were 63% in LBW and 37% in more than 2.5 kg. Taksande et al 16 found that the percentage of neonatal seizure was more in LBW babies (57.3%) than the babies with birth weight more than 2.5 kg.( 42.7%). In our study 65.6 % cases had seizures during first 3 days (72 hours) of life and hypoxic ischemic encephalopathy (HIE) remained the main etiological factor in 37.6% cases. Calciolari et al 17 in his study reported that 73.30% cases had seizures during the first two days of life and Hypoxic- Ischemic-encephalopathy was the main etiological factor found in 79.09% cases. In a study by Arvind Sood18 54.23% cases had seizures during first 3 days of life and Hypoxic-Ischemic-Encephalopathy was the main etiological factor, which is similar to our findings. Coen RW etal19 found that 81% of babies had early onset seizures (<72hrs). In our study 62% cases had single seizure type and combined type of seizures were observed in 38 % of cases. In single type seizure subtle seizures were commonest 30.8%. Calciolari et al 17 reported single seizure type in 50% of cases and combined type in 50% and among the single type, subtle seizure were more common in 21% cases. Arvind Sood18 in his study had 69.49% cases with single seizure type and subtle seizures being the most common among them in 27.11% of cases.
In our study 38.8% had seizures due to hypoxic ischemic encephalopathy (HIE) followed by infection found in 29.2 % number of cases, metabolic abnormalities were found in 20.4% cases. Taksande et al16 and Arvind Sood18 had similar results regarding HIE as main cause but in some studies metabolic seizures were more common than infection as etiology for seizures. Other etiological factors found in the present study were intraventricular hemorrhage, kernicterus and developmental defects. Fifth day fit, Infarction and Familial were not found in our study. In this study biochemical abnormalities were seen both in primary metabolic seizures and non metabolic seizures, hypoglycemia was commonest biochemical disturbance followed by hypocalcaemia, hyponatremia and hypomagnesaemia in both. Hypoglycemia and hypocalcaemia was commonest in Hypoxic ischemic encephalopathy, and hypoglycemia and hyponatremia were common in sepsis and meningitis cases with neonatal seizures.
Subtle seizures were the most common seizures in hypocalcaemia and hypomagnesaemia while multifocal clonic seizures were the most common type in hypoglycemia and hyponatremia.
In our study 26% cases died and 74% were discharged, HIE remained the leading cause of death in cases with neonatal seizures in Term neonates, while in preterm neonates Sepsis and IVH were the leading cause. Our findings are comparable with the study done by Nunes ML et al 20 who found that 24.7% of the cases died in the neonatal period. In a study done by G.Sahana et al21 18.35% neonates died. Our study has a little higher percentage of neonatal deaths and it could be attributed to the severity of the etiological factors in our cases of neonatal seizures.
Conclusion:
Overall incidence of neonatal seizures in our study was 3.27%. Male: Female ratio was 1.27:1
The study shows much higher incidence of neonatal seizures in preterm babies (14.35%) and low birth weight babies (8.19%). Underlying maternal diseases were seen in 50.8% babies with neonatal seizures. Subtle seizure represents the commonest type of neonatal seizure found in our study in both term and preterm neonates. Neonatal seizures are most common in first three days of life. Hypoxic ischemic encephalopathy was the most common cause of neonatal seizures seen in 34.4%.cases followed by Infection. Biochemical abnormalities are common in neonatal seizures.
Primary biochemical abnormalities without other co- morbid states which could account for the seizures are seen in 20.4 %. Hypoglycemia and hypocalcaemia are the commonest biochemical abnormalities accounting for seizures in this group. In non metabolic group 25.2% of cases of neonatal seizures with identifiable etiology had biochemical abnormality. Among biochemical abnormality subtle seizures are most common in hypocalcaemia and hypomagnesaemia while hypoglycemia and hyponatremia had multifocal seizures as most common type. A significant high mortality rate was associated with Hypoxic ischemic encephalopathy
Recommendations:
Good Antenatal care and early diagnosis of chronic illnesses in mother with proper management is necessary. “Late preterm” babies should be always examined and monitored with more caution. Low birth weight babies are more vulnerable for neonatal seizures. Prevention of Low Birth Weight babies (IUGR and Preterm) could be done by improved antenatal care and monitoring of these neonates in NICU. Facilities for Neonatal resuscitation, prevention of Birth Asphyxia and safe deliveries are mandatory at all levels of health care systems. The medical and paramedical staff should also be trained in anticipating, monitoring and observation for subtle seizures and treatment protocols of neonatal seizures.
Limitations:
A longitudinal follow up was not done; EEG and neuroimaging could not be done.
Contribution: AK – concept, monitoring, clinical decisions, JV – Guidance, Ethical issues, approval of final manuscript. NT – Clinical work, review of literature, initial manuscript.
Conflict of Interest: None
Source of Funding: Nil
Underlying maternal diseases were seen in 50.8% babies with neonatal seizures.
Neonatal seizures are most common in first three days of life.
Primary biochemical abnormalities without other co- morbid states which could account for the seizures are seen in 20.4 %. Hypoglycemia and hypocalcaemia are the commonest biochemical abnormalities.
References:
1) Mizrahi Eli M. Neonatal Seizures and neonatal epileptic syndromes. Neurologic clinics in epilepsy 2001;19(2):427-456.
2) Holden KR, Freeman JM. Neonatal seizures and their treatment. ClinPerinatol 1975;2: 3- 13.
3) Garg PK. Neonatal seizures. Indian J. Pediatrics 1972;39:208-13.
4) Zupana ML. Neonatal seizures. Pediatric Clinics of N America 2004; 51: 961-978.
5) Airede KI. Neonatal seizures and a 2 year neurological outcome. J Trop Pediatr1991; 37: 313-17.
6) Rose A LA, Lombroso CT. A study of clinical, pathological and electroencephalographic features in 137 full term babies with a long term follow up. Pediatrics 1969; 45: 404-25.
7) Hill A, Volpe JJ. Neurologic disorders. In:Avery GB, Flctcher MA, Macdonald MG,editors. Neonatology, pathophysiology and management of the newborn. 4th ed .Philadelphia:JB Lippincott company; 1994.p.1117-39.
8) Bagla et al. Clinicoetiology profile of neonatal seizures Indian J Child Health 2017;4(3):383-386.
9) National Neonatal Perinatal Database. National Neonatology Forum, India. Report for year 2002-03.
10) Cockburn F, Brown JK, Belton NR, Forfar JO. Neonatal convulsions associated with primary disturbance of calcium, phosphorus and magnesium metabolism. Arch Dis Childhood 1973; 48:99-108.
11) Fredrichsen C. Tetany in a sucking infant with latent osteitisfibrosa in the Mother. Lancet 1939;1:85.
12) Intyrel MC, Boss S, Troughton VA. Parathyroid hormones and magnesium homeostasis. Nature 1963 ;198 :1058-60.
13) Gabriel M, Ronen, Sharon Penny, Wayne Andrews. The epidemiology of clinical neonatal seizures in New Found land: A population based study. J Pediatr 1999; 134: 71-75.
14) Kumar A, Gupta A and Talukdar B. Clinicoetiological and EEG profile of neonatal seizures. Indian J Pediatr2007;74(1):33-37.
15) Holden KR, Freeman JM. Neonatal seizures and their treatment. ClinPerinatol 1975;2:3- 13.
16) Taksande A, Vilhecar K, Jain M, Lakra M. Clinico Biochemical Profile of Neonatal Seizures. Indian J Pediatr1995?52:424-7.
17) Calciolari G, Perlman JM, Volpe JJ. Seizures in the neonatal intensive care unit of the 1980s. Clinical Pediatr1988; 27: 119-123.
18) Sood A, Grover N, Sharma R. Biochemical abnormalities in neonatal seizures. Indian. Journal of pediatrics 2003; 70: 221-224.
19) Coen RW, Mc Cutchen CB, WarmaDet al. Continuous monitoring of electroenc ephalogram following perinatal asphyxia. J Pediatr 1982; 100: 628-630.
20) Nunes ML, Martins MP, RicardoCMB. JadersonW. Neurological outcome of Newborns with NeoNatal seizures. Arq Neuropsiquiatr 2008; 66(2-A):168-174. G. Sahana*, B. Anjaiah. Clinical profile of neonatal seizures.IJMAS2014; 1(3): 2320?3137.
Issue: January-March 2018 [Volume 7.1]