Abstract:
Introduction: The children of migrant population like Brick-kiln workers, construction site workers etc receive least attention as regards assessment of their nutritional status and planning and implementing nutritional interventional programmes especially in rural areas. Objectives: 1) To assess the nutritional status by Anthropometric means in 1-5 year old children of Brick-kiln workers at rural areas of taluka Panvel 2) To assess the prevalence of clinical signs of major nutritional deficiencies. Material and methods: A communitybased, cross-sectional study was conducted at Brick-kilns of Targhar and Pargoan villages which are the rural areas in Taluka Panvel during February to April 2014. A total of 161 children of Brick-kiln workers in age group 1-5 years were randomly selected using simple random sampling. Parents were interviewed using a pretested questionnaire regarding the immunization status, milestones, complaints and medical illness. The children were clinically examined for signs of nutritional deficiencies and anthropometrically assessed. The data was compared with WHO/NCHS standards to assess malnutrition in the study group. Statistical analysis was done using Z score, Mean and Percentage using SPSS 17.0. Results: The major nutritional deficiencies found were Pallor (54.80 %), Angular stomatitis (17.78%), Glossitis (14.56 %) and Vitamin A deficiency (8.10 %). The prevalence of malnutrition (below 2SD) in terms of underweight, stunting and wasting was observed in 62.3%, 51.2% and 36.4 % children respectively. Severe degree (below -3SD) of underweight, stunting and wasting was observed in 28.9 %, 25.6 % and 7.1 % children respectively. The immunization status was found poor. Conclusion: The study revealed poor immunization status, malnutrition and nutritional deficiencies in children of Brick kiln workers. There is an urgent need for strengthening the health and nutritional interventional programmes for children of migratory population.
Keywords: Brick-kiln workers, Anthropometric assessment, Malnutrition, Rural areas.
Introduction:
Globally, one in four children under five yearold are stunted, 16% are underweight and 8% are wasted 1. The Millennium Development Goal target is to halve it by 2015 however as per the present trends these targets will be missed by 30 million children 2.Malnutrition continues to be a public health problem, particularly among vulnerable groups such as pre-school children, pregnant and lactating women, despite dramatic increase in food production at national level. The World Bank estimates that India is ranked second following Bangladesh in producing the malnourished children globally 3. India accounts for about 40% of undernourished children in the world, which contribute to high morbidity and mortality in the country 4. In addition it is estimated that more than one-third of under five deaths are attributable to under nutrition 5. This implies persistence of poverty and malnutrition in the country. In spite of its remarkable economic growth in the past decade, India’s progress in reducing child malnutrition has been exclusively slow.
Assessment of Nutritional status is necessary for early detection of malnutrition and for assessing the effectiveness of preventive programmes. Anthropometry is widely recognized as one of the useful techniques to assess the growth and nutritional status of an individual or population 6, 7. One of the basic reasons is that anthropometry is highly sensitive to under nutrition 8. Malnutrition is frequently part of a vicious cycle that includes poverty and disease. The 3 factors, viz., malnutrition, poverty and disease are interlinked in such a way that each contributes to the presence and permanence of the others.
Studies have demonstrated that the more malnourished children are, the sicker they are and the higher their risk of early death 9, 10, 11. Severe malnutrition leads not only to increased morbidity and mortality, but can also lead to impaired psychological and intellectual development. Growth retardation in early childhood, for example, has been linked to the delayed acquisition of motor skills 12 and to delayed mental development 13.
This problem is much more severe in children of migratory population such as brick-kiln workers, building-construction workers, tribal population who are skipped out often from the National nutritional interventional programmes. A majority of the workers at brick-kilns are migrant laborers from impoverished areas who earn low wages, live under miserable conditions and are prone to various diseases, including malnutrition. Their children are at increased risk of suffering from malnutrition because of various reasons such as, restricted access to health services, lack/poor medical facilities, poverty, recurrent infections, lack of nutritious food, illiteracy and ignorance about nutrition and health care. Various supplementary feeding programmes do exist in India, but they miss out the nomadic population such as Buildingconstruction workers, Brick-Kiln workers. The migratory nature of their occupation, poses a hurdle in assessing the nutritional status of children of Brick kiln workers and in planning and implementing nutritional interventional programmes. With this background this study was conducted to assess the nutritional status by anthropometric assessment and assess the clinical morbidities and major nutritional deficiencies among 1-5 year old children of Brick-kiln workers at rural areas of Taluka Panvel, dist. Raigad.
Materials and Methods:
A cross sectional community based study was conducted at a Brick-kilns of Targhar and Pargoan villages which are the rural areas in Taluka Panvel, District Raigad during February to April 2014. Total of 161 children in age group 1-5 years were taken by complete enumeration as the study subjects. Out of 161 study subjects, 67 are from Targhar and 94 are from Pargoan.
Ethical approval was taken from the Institutional Ethical committee. A predesigned, structured questionnaire was prepared in English and validated. Pilot study was conducted among 25 study subjects. Written informed consent was taken from the parents of the study subjects after discussing the aim of the study. Children between 1 to 5 years of age group who were to remain in these brick kilns during the study period were all included for the study where as those children who were severely ill and those whose parents were not willing to participate in the study or those who migrated were excluded from the study.
Parents were interviewed using a pretested questionnaire regarding the immunization status, milestones, complaints and medical illness. The children were clinically examined for signs of nutritional deficiencies and anthropometrically assessed. The data was compared with WHO standards to assess malnutrition in the study group. The three most commonly used internationally recommended anthropometric indicators are stunting (low height-for-age), underweight (low weight- for-age) and wasting (low weight-for height) 14.
Malnutrition was assessed using the criteria of Weight-for-age(W/A), Height-for Age(H/A) and Weight-for-Height(W/H). A low weight-for-age (W/A) is considered to indicate underweight and, in the absence of significant wasting in a community, like low height-for-age (H/A), reflects sub-optimal long term health and nutritional conditions. A low height-for-age (H/A) indicates stunting, and reflects a process of failure to reach linear growth potential as a result of sub-optimal health and/ or nutritional conditions. A low weight-for height (W/H) indicates wasting, and reflects in most cases a recent and severe process of weight loss, which is associated with acute starvation and/or severe disease. Statistical analysis was done using Z score, Mean and Percentage using SPSS version 21.0.
Results and Discussions:
In the present study the participants were children of 1 to 5 years of Brick kiln workers from Targhar and from Pargoan.
{kind=link}
In the present study, the prevalence of under nutrition ( below 2SD ) in terms of underweight, stunting and wasting was observed in 61.9%,49.5%,and 35.7% children respectively. Severe degree ( below -3SD) of underweight, stunting and wasting was observed in 27.3%,24.2% and 5.9% children respectively.
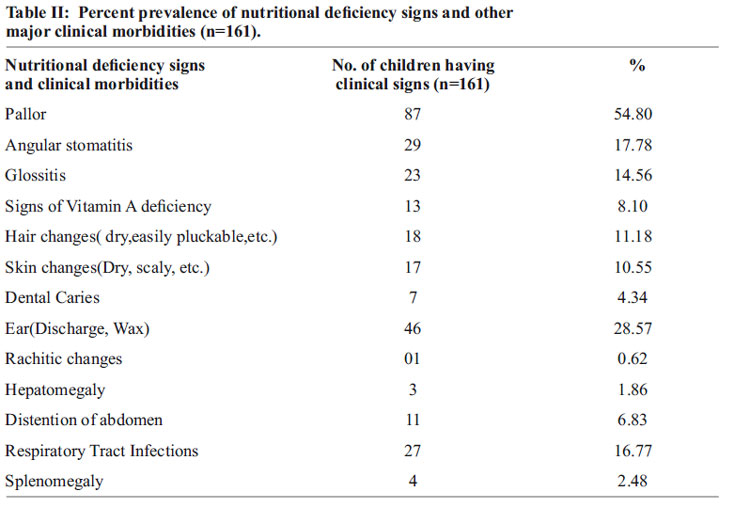
The major nutritional deficiencies found were Pallor (54.80 %), Angular stomatitis (17.78%), Glossitis (14.56 %) Vitamin A deficiency (8.10 %)
{kind=link}
The present study also highlighted poor immunization status of these children.
Only 23.52 % were immunized with BCG vaccine, 27.45 % children with OPV and DPT vaccines, 24.18 % and 25.49 % children with measles vaccine and Vitamin A doses respectively.
Conclusion: Thus the study revealed widespread prevalence of malnutrition, nutritional deficiency signs and clinical morbidities in the children of Brick-kiln workers. The study revealed poor immunization status of children.
Recommendations:
Thus there is an urgent need for strengthening the existing health and nutritional programmes which will help to reduce the prevalence of malnutrition in such children of migratory population and thereby reducing child morbidity and mortality.
Funding- Nil
Object of Interest – Nil
Contribution of Authors- Kiran H. Mali- Clinical Work and statistics.
Pradeep Sawardekar- Manuscript writing Seema Anjeneya- Concept and Guidance
References:
1. UNICEF Global Nutrition Database, 2012. Based on Multiple Indicator Cluster Surveys (MICS), Demographic and Health Surveys (DHS) and other national surveys).
2. United Nations, The Millennium Development Goals Report 2007, United Nations Department of Economic and Social Affairs, New York, June 2007, Pp. 4.
3. India Country overview 2009; World Bank Report [online]. 2011 [cited 2009 November 11]. Available from: http://www. worldbank .org.
4. James LF. India sector review of nutrition programmes, a back ground paper prepared for the World Bank, New Delhi, 1998.
5. Liu et al, 2012;Black et al, 2008( http://www. scalingupnutrition.org/.) [Citation date: 23/12/2014]
6. Gorstein, J., Sullivan, K., Yip, R., de Onis, M., Trowbridge, F. and Fajans, P.: Issues in assessment of nutritional status using anthropometry. Bulletin of WHO, 72: 272-283 (1994).
7. Rao, K.V., Balakrishna, N. and Adinarayana, K.: Critical limits of some anthropometric measurements and indices for the assessment of nutritional status. J. Nutr. Dietet., 23: 88-99 (1986).
8. Martorell, R. and Ho, T.J.: Malnutrition, morbidity and mortality. Popul. Dev. Rev., 10 (Suppl.): 49-68 (1984).
9. Pelletier D (1991). Relationships between child anthropometry and mortality in developing countries. Ithaca, NY, Cornell University (Cornell Food and Nutrition Policy Program, Monograph 12).
10 Toole MF, Malkki RM (1992). Famineaffected, refugee, and displaced populations: recommendations for public health issues. Morbidity and Mortality Weekly Report, 41:1?25.
11. Man WD, Weber M, Palmer A, Schneider G, Wadda R, Jaffar S, Mulholland EK, Greenwood BM (1998). Nutritional status of children admitted to hospital with different diseases and its relationship to outcome in The Gambia, West Africa. Tropical Medicine and International Health, 3:678?686.
12. Heywood AH, Marshall T, Heywood PF (1991). Motor development and nutritional status of young children in Madang, Papua New Guinea. Papua New Guinea Medical Journal, 34:109?116.
13. Mendez MA, Adair LS (1999). Severity and timing of stunting in the first two years of life affect performance on cognitive tests in late childhood. Journal of Nutrition, 129:1555 ?1562.
14. Physical status: the use and interpretation of anthropometry, Geneva: World Health Organization; 1995. Report of a WHO Expert Committee. Technical Report Series, No. 854.
Issue: October-December 2017 [Volume 6.4]